Symptom finder - The causes of polyuria
Symptom finder - The causes of polyuria
Definition of polyuria is the production of urine /urine output of more than 3 liters within 24 hours.
The causes of polyuria are excessive intake of fluid which can be psychogenic, any anticholinergic intake ( drug induced thirst ) and hypothalamic disease.
Diabetes insipidus is the major cause of polyuria. There are 2 forms of diabetes insipidus such as nephrogenic diabetes insipidus and cranial diabetes insipidus. Nephrogenic diabetes insipidus may be X linked inherited disorder, due to chronic hypercalcemia, hypokalemia, recovering obstructive uropathy, drugs ( democycline, lithium) , recovering acute tubular necrosis and chronic tubulointerstitial nephritis.
Cranial diabetes insipidus is causes by drugs ( opiates), sarcoidosis or tuberculosis ( pituitary granuloma), recessive or dominant inheritance, neurosurgery, idiopathic deficiency of production of ADH, head injuries and pituitary brain tumor.
Polyuria may also be caused by osmotic diuretic condition such as urea, mannitol, hyperglycemia and hypercalcemia or therapeutic diuretic condition such as the intake of amiloride, bendrofluazide and frusemide. Type 1 and type 2 diabetes mellitus, hypercalcemia and diabetes insipidus may present with polyuria and polydipsia.
Insensible loss , physiological requirement and amount of fluid intake will influence the volume of urine produced per day in each individual.
Generally, it is important to differentiate between frequency of micturition ( passing frequently of urine in small amount) and polydipsia ( passing large volume of urine frequently) . Polyuria and polydipsia usually occur at the same time . Polydipsia is an excessive water intake and in case of polyuria, polydipsia is useful to replace all water that has loss. Polydipsia is activated by thirst.
Osmotic diuresis is the common features of diabetes mellitus/hyperglycemia . In this case polyuria and polydipsia are commonly present at the same time. Family hisotry of diabetes insipidus is vital as diabetes insipidus is an inherited disorder. Multiple myeloma, gout, polycystic kidney disease and reflux nephropathy may lead to chronic tubulointerstitial nephritis ( causes of polyuria). Acute tubular necrosis is commonly present due to hemorrhage or sepsis from renal ischemia.
Hypercalcemia due to hyperparathyroidism or malignancy may cause polyuria by development of nephrogenic diabetes insipidus or intrinsic osmotic diuresis effect. Cranial diabetes insipidus is caused by craniopharyngioma, neurosurgery ( transient post complication), pineal gland tumor and severe blunt , trauma to the head.
The investigations require are serum glucose, serum calcium, urea and electrolytes, urine and plasma osmolality, urine dipstick and 24 hour urine collection. The purpose of these tests are to differentiate between diabetes insipidus, excessive intake of fluid and osmotic diuresis.
Definition of polyuria is the production of urine /urine output of more than 3 liters within 24 hours.
The causes of polyuria are excessive intake of fluid which can be psychogenic, any anticholinergic intake ( drug induced thirst ) and hypothalamic disease.
Diabetes insipidus is the major cause of polyuria. There are 2 forms of diabetes insipidus such as nephrogenic diabetes insipidus and cranial diabetes insipidus. Nephrogenic diabetes insipidus may be X linked inherited disorder, due to chronic hypercalcemia, hypokalemia, recovering obstructive uropathy, drugs ( democycline, lithium) , recovering acute tubular necrosis and chronic tubulointerstitial nephritis.
Cranial diabetes insipidus is causes by drugs ( opiates), sarcoidosis or tuberculosis ( pituitary granuloma), recessive or dominant inheritance, neurosurgery, idiopathic deficiency of production of ADH, head injuries and pituitary brain tumor.
Polyuria may also be caused by osmotic diuretic condition such as urea, mannitol, hyperglycemia and hypercalcemia or therapeutic diuretic condition such as the intake of amiloride, bendrofluazide and frusemide. Type 1 and type 2 diabetes mellitus, hypercalcemia and diabetes insipidus may present with polyuria and polydipsia.
Insensible loss , physiological requirement and amount of fluid intake will influence the volume of urine produced per day in each individual.
Generally, it is important to differentiate between frequency of micturition ( passing frequently of urine in small amount) and polydipsia ( passing large volume of urine frequently) . Polyuria and polydipsia usually occur at the same time . Polydipsia is an excessive water intake and in case of polyuria, polydipsia is useful to replace all water that has loss. Polydipsia is activated by thirst.
Osmotic diuresis is the common features of diabetes mellitus/hyperglycemia . In this case polyuria and polydipsia are commonly present at the same time. Family hisotry of diabetes insipidus is vital as diabetes insipidus is an inherited disorder. Multiple myeloma, gout, polycystic kidney disease and reflux nephropathy may lead to chronic tubulointerstitial nephritis ( causes of polyuria). Acute tubular necrosis is commonly present due to hemorrhage or sepsis from renal ischemia.
Hypercalcemia due to hyperparathyroidism or malignancy may cause polyuria by development of nephrogenic diabetes insipidus or intrinsic osmotic diuresis effect. Cranial diabetes insipidus is caused by craniopharyngioma, neurosurgery ( transient post complication), pineal gland tumor and severe blunt , trauma to the head.
The investigations require are serum glucose, serum calcium, urea and electrolytes, urine and plasma osmolality, urine dipstick and 24 hour urine collection. The purpose of these tests are to differentiate between diabetes insipidus, excessive intake of fluid and osmotic diuresis.
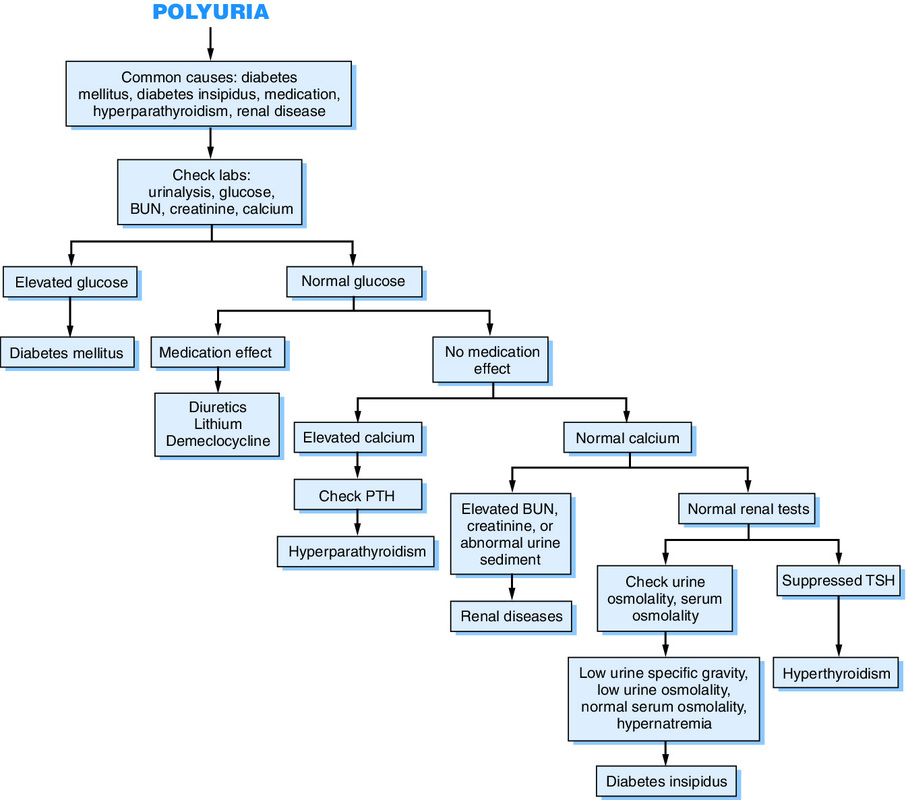
Serum glucose will rise in diabetes mellitus. Raised serum calcium is associated with osmotic diuresis which is related to chronic tubulointerstitial nephritis. Urea and electrolytes may reveal low potassium in nephrogenic diabetes insipidus. Polydipsia ( excessive fluid intake ) is characterized by low urea, low creatinine and low sodium. Renal failure present with raised plasma creatinine and urea levels. Uncompensated polyuria without any adequate intake of water may lead to raised sodium level. Urine dipstick is important to detect the present of glucose in diabetes mellitus. Urinary frequency is differentiated from polyuria by performing the 24 hour urine collection studies. Polyuria is confirmed id more than 3 liters of urine are produced in 24 hour urine collection test. Pituitary /cranial and nephrogenic diabetes insipidus are confirmed by low urine osmolality and normal /raised plasma osmolality. In polydipsia ( compulsive drinking ) there will be low urine osmolality and normal or low plasma osmolality.
Water deprivation test and DDAVP test are useful to differentiate between diabetes insipidus and primary polydipsia.
Water deprivation test is performed by restriction of water intake overnight and measurement of plasma osmolality as well as urine osmolality. The test is not performed in case of hypernatremia or patient with severely depleted volume of body fluid. Low plasma osmolality indicates the present of primary polydipsia. Raised plasma osmolality is an indication of the need to measure urine osmolality and stop the measurement of plasma osmolality. Low urine osmolality may confirm diabetes insipidus if performed on three consecutive samples. Raised urine osmolality indicates no diabetes insipidus. DDAVP test is considered by adding arginine vasopressin . If there is no raised in urine osmolality then neprhogenic diabetes insipidus is confirmed. If there is raised urine osmolality, then cranial diabetes insipidus is confirmed.
Other specific investigations are CT - scan /MRI - scan of the head to rule out hypothalamic disease and tumor. Renal biopsy is performed to rule out chronic tubulointerstitial nephritis and acute tubular necrosis.
Water deprivation test and DDAVP test are useful to differentiate between diabetes insipidus and primary polydipsia.
Water deprivation test is performed by restriction of water intake overnight and measurement of plasma osmolality as well as urine osmolality. The test is not performed in case of hypernatremia or patient with severely depleted volume of body fluid. Low plasma osmolality indicates the present of primary polydipsia. Raised plasma osmolality is an indication of the need to measure urine osmolality and stop the measurement of plasma osmolality. Low urine osmolality may confirm diabetes insipidus if performed on three consecutive samples. Raised urine osmolality indicates no diabetes insipidus. DDAVP test is considered by adding arginine vasopressin . If there is no raised in urine osmolality then neprhogenic diabetes insipidus is confirmed. If there is raised urine osmolality, then cranial diabetes insipidus is confirmed.
Other specific investigations are CT - scan /MRI - scan of the head to rule out hypothalamic disease and tumor. Renal biopsy is performed to rule out chronic tubulointerstitial nephritis and acute tubular necrosis.
