
Emergency Strategy - How to treat the fracture of the clavicle
Emergency Strategy- How to treat fracture of the clavicle
Patient who suffer from the fracture of clavicle is admitted to the hospital if the condition is life threatening and the patient presented with open fractures. Initial treatment may include assessment of the patient’s airway, breathing and circulation. NSAIDS is given to the patient. Pack of ice is applied to the affected area. The affected area is also immobilize with a sling.
There are two different form of fractures known as closed fracture and open fracture. Open fracture may require internal fixation and open debridement while closed fracture may require closed reduction and immobilization at the sites of fracture. Open fracture is a rare and serious condition.
In case of proximal third of clavicle fracture ( closed fracture), the treatment include administration of NSAIDS as pain reliever, ice pack to the affected area for 24 hours and immobilizer with shoulder immobilize or splint. Further orthopedic assessment is required.
In case of middle third of clavicle fracture ( closed fracture), the treatment include administration of NSAIDS, ice pack to the affected area for 24 hours, a sling, figure eight splint or shoulder immobilizer should be applied for support. Patient may be sedated to relieve anxiety and pain. Close reduction may be performed. The procedure involved pulling the shoulder backward, upward and outward. 1% of lidocaine is administrated to the hematoma at the sites of fracture.
In case of distal third fracture of the clavicle , the treatment may include administration of NSAIDS as pain reliever, ice pack at the sites of fracture for 24 hours, sling/shoulder immobilizer for immobilization, practice different form of range of movement or considering orthopedic assessment in severe/serious cases.
Patient will be discharge if the patient only suffer closed fracture with adequate management of pain. Good home support is also important.Follow up at orthopedic clinic is important. During follow up, patient’s range of motion and neurological status is assessed ( motor and sensory function). Any evidence of cardiopulmonary compromise or cervical spinal cord injury may require admission.
Patient with fracture of the clavicle may present with signs which is detectable by performing physical examination. On inspection, the physician may notice the displacement of the shoulder anteriorly and posteriorly.Crepitus will be heard. Tenderness and swelling are localized to the site of fractures. Clavicle, shoulder and humerus are examined to look for any evidence of fracture, swelling, subluxations and dislocations . Observe for other related injuries such as injuries to the cervical spine, injury of the aortic arch due to fracture of the first rib. Fracture, dislocation and separation of the acriomioclavicular joint and sternoclavicular joint. It is also important to observe for any evidence of closed or open fractures and conduct the full neurological examination.
Clavicular fracture may involved medial fracture which affect the sternoclavicular separation and distal fracture which leads to separation of the acriomioclavicular separation.
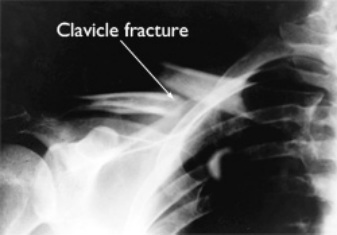
Radiography is an important diagnostic studies. Radiography studies may rule out shoulder fracture or dislocation. There are three different views that can be taken from radiography such as AP view of both clavicles, upper lung field ( to rule out pneumothorax) and shoulder girdle ( to rule out fracture of the shoulder). Weight bearing /stress view are rarely performed to rule out distal fracture of the clavicle. Medial and distal clavicular fracture are best detected with oblique and apical lordotic view. Any vascular injuries especially subclavian vessel are best detected with angiography.
There are three different group of clavicular fracture. Group 1 is associated with middle third fracture which is the most common cause of clavicular fracture. Group II clavicular fracture that involved distal third of clavicle are further divided into Type 1 where the coracoclavicular ligament remain undisplaced and intact.Type II may lead to severing of the coracoclavicular ligament while type III involve the acromioclavicular joint articular surface. Group III is the proximal third part of clavicle fracture. Group III clavicle fracture is the least common. Clavicular fracture most commonly affects the neonates due to trauma at birth . Clavicular fracture also the most common cause of fracture in children.
The common causes of clavicular fractures are fall on the outstretched hand, fall on the lateral shoulder and trauma directly to the clavicle.
References
1.Post, M. “Current Concepts in the Treatment of Fractures of the Clavicle.” Clinical Orthopaedics and Related Research no. 245 (August 1989): 89–101.
2.Zlowodzki, Michael, Boris A Zelle, Peter A Cole, Kyle Jeray, Michael D McKee, and Evidence-Based Orthopaedic Trauma Working Group. “Treatment of Acute Midshaft Clavicle Fractures: Systematic Review of 2144 Fractures: On Behalf of the Evidence-Based Orthopaedic Trauma Working Group.” Journal of Orthopaedic Trauma 19, no. 7 (August 2005): 504–507.
3.Kona, J, M J Bosse, J W Staeheli, and R L Rosseau. “Type II Distal Clavicle Fractures: a Retrospective Review of Surgical Treatment.” Journal of Orthopaedic Trauma 4, no. 2 (1990): 115–120.
Patient who suffer from the fracture of clavicle is admitted to the hospital if the condition is life threatening and the patient presented with open fractures. Initial treatment may include assessment of the patient’s airway, breathing and circulation. NSAIDS is given to the patient. Pack of ice is applied to the affected area. The affected area is also immobilize with a sling.
There are two different form of fractures known as closed fracture and open fracture. Open fracture may require internal fixation and open debridement while closed fracture may require closed reduction and immobilization at the sites of fracture. Open fracture is a rare and serious condition.
In case of proximal third of clavicle fracture ( closed fracture), the treatment include administration of NSAIDS as pain reliever, ice pack to the affected area for 24 hours and immobilizer with shoulder immobilize or splint. Further orthopedic assessment is required.
In case of middle third of clavicle fracture ( closed fracture), the treatment include administration of NSAIDS, ice pack to the affected area for 24 hours, a sling, figure eight splint or shoulder immobilizer should be applied for support. Patient may be sedated to relieve anxiety and pain. Close reduction may be performed. The procedure involved pulling the shoulder backward, upward and outward. 1% of lidocaine is administrated to the hematoma at the sites of fracture.
In case of distal third fracture of the clavicle , the treatment may include administration of NSAIDS as pain reliever, ice pack at the sites of fracture for 24 hours, sling/shoulder immobilizer for immobilization, practice different form of range of movement or considering orthopedic assessment in severe/serious cases.
Patient will be discharge if the patient only suffer closed fracture with adequate management of pain. Good home support is also important.Follow up at orthopedic clinic is important. During follow up, patient’s range of motion and neurological status is assessed ( motor and sensory function). Any evidence of cardiopulmonary compromise or cervical spinal cord injury may require admission.
Patient with fracture of the clavicle may present with signs which is detectable by performing physical examination. On inspection, the physician may notice the displacement of the shoulder anteriorly and posteriorly.Crepitus will be heard. Tenderness and swelling are localized to the site of fractures. Clavicle, shoulder and humerus are examined to look for any evidence of fracture, swelling, subluxations and dislocations . Observe for other related injuries such as injuries to the cervical spine, injury of the aortic arch due to fracture of the first rib. Fracture, dislocation and separation of the acriomioclavicular joint and sternoclavicular joint. It is also important to observe for any evidence of closed or open fractures and conduct the full neurological examination.
Clavicular fracture may involved medial fracture which affect the sternoclavicular separation and distal fracture which leads to separation of the acriomioclavicular separation.
Radiography is an important diagnostic studies. Radiography studies may rule out shoulder fracture or dislocation. There are three different views that can be taken from radiography such as AP view of both clavicles, upper lung field ( to rule out pneumothorax) and shoulder girdle ( to rule out fracture of the shoulder). Weight bearing /stress view are rarely performed to rule out distal fracture of the clavicle. Medial and distal clavicular fracture are best detected with oblique and apical lordotic view. Any vascular injuries especially subclavian vessel are best detected with angiography.
There are three different group of clavicular fracture. Group 1 is associated with middle third fracture which is the most common cause of clavicular fracture. Group II clavicular fracture that involved distal third of clavicle are further divided into Type 1 where the coracoclavicular ligament remain undisplaced and intact.Type II may lead to severing of the coracoclavicular ligament while type III involve the acromioclavicular joint articular surface. Group III is the proximal third part of clavicle fracture. Group III clavicle fracture is the least common. Clavicular fracture most commonly affects the neonates due to trauma at birth . Clavicular fracture also the most common cause of fracture in children.
The common causes of clavicular fractures are fall on the outstretched hand, fall on the lateral shoulder and trauma directly to the clavicle.
References
1.Post, M. “Current Concepts in the Treatment of Fractures of the Clavicle.” Clinical Orthopaedics and Related Research no. 245 (August 1989): 89–101.
2.Zlowodzki, Michael, Boris A Zelle, Peter A Cole, Kyle Jeray, Michael D McKee, and Evidence-Based Orthopaedic Trauma Working Group. “Treatment of Acute Midshaft Clavicle Fractures: Systematic Review of 2144 Fractures: On Behalf of the Evidence-Based Orthopaedic Trauma Working Group.” Journal of Orthopaedic Trauma 19, no. 7 (August 2005): 504–507.
3.Kona, J, M J Bosse, J W Staeheli, and R L Rosseau. “Type II Distal Clavicle Fractures: a Retrospective Review of Surgical Treatment.” Journal of Orthopaedic Trauma 4, no. 2 (1990): 115–120.
