
Emergency Strategy - How to treat Carpal tunnel syndrome
Emergency Strategy - How to treat Carpal tunnel syndrome
Treatment for carpal tunnel syndrome can be based into treatment of acute carpal tunnel syndrome and treatment of chronic carpal tunnel syndrome . Surgical decompression procedure is required in case of acute carpal tunnel syndrome while pain control and management are suitable for chronic cases of carpal tunnel syndrome.
In acute case of carpal tunnel syndrome, after making sure that the airway, breathing and circulation remain intact, the patient is refer to the hand surgeon. Hand surgeon will perform endoscopically or open surgical release of transverse carpal ligament.
In chronic case of carpal tunnel syndrome, surgical release of transverse carpal ligament may also be performed by hand surgeon open or endoscopically. Patient is advised to avoid any repetitive movement of the wrist. Visit to occupational therapist is important as nerve gliding exercises or tendon gliding exercise and ergometric testing can be performed. Local injection of corticosteroid , NASIDS or aspirin can also be given. The patient’s wrist is splint in a neutral position . The splint of the wrist is worn during night time.
Carpal tunnel syndrome can be an acute or chronic cases. Carpal tunnel syndrome may present as pain in the hand or wrist which radiates to the shoulder, elbow and forearm. The pain is exacerbated by exercise or activity which involved repetitive movement of the wrist, flexing the wrist or driving. The pain is also sever at night and relived by shaking the hand. Besides pain, patient may complain of paraesthesia, which affect the thumb, middle f, index fingers and radial aspect of the finger. Paraesthesia mostly affect the distribution of the median nerve. Loss of sensaton and loss of 2 points of discrimination may occur. Wasting and atrophy of the thenar muscle may present. Weakness of muscles are commonly affecting the opponens pollicis and abductor pollicis brevis muscles. Patient will complain of decrease fine motor control and hand dropping. Both of these muscles are innervated by median nerve.
Other tests include tourniquet test, carpal compression test and Tinel test. In tourniquet test, paraesthesia may occur after 2 minutes of inflation of the cuff to a pressure 2 mmHg above the patient systolic pressure. Tingling in the finger may occur after direct pressure is applied to the proximal part of carpal tunnel ligament in distribution of median nerve. This is known as carpal compression test. Tinel test is associated with tingling sensation after tapping the wrist over the distribution of the median nerve.
The common differential diagnosis of carpal tunnel syndrome are brachial plexitis, thoracic outlet obstruction, syringomyelia, first carpometacarpal joint osteoarthritis, cervical nerve root compression ( worst by movement of the neck or erect posture) and hand - arm vibration syndrome ( upper extremities myalgia, grip weakness, tingling and numbness when exposed to vibration and cold in the ulnar and median nerve distribution and present of Raynaud’s phenomenon.
Investigations required are analysis of rheumatoid factor, thyroid function test and immunological analysis. Fracture or arthritis degeneration in nature is detected by radiography of the wrist. Ultrasound may reveal transcarpal ligament bowing, flattening of median nerve at distal canal and swelling of the median nerve at proximal canal. MRI scan may reveal the present of fluid in the carpal tunnel, transcarpal ligament bowing, swelling of the synovium and median nerve. Carpal tunnel encroachment may be detected with CT scan. Other specific test include electromyography and nerve conduction test.
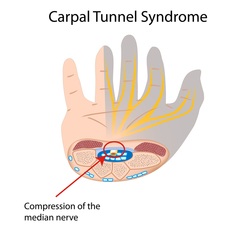
What is carpal tunnel? Carpal tunnel is an area bound by transverse carpal ligament and carpal bone. Inside carpal tunnel, there are flexor pollicis longus, median nerve, flexor digitorum profundus and flexor digitorum superficialis .
What is carpal tunnel syndrome ? Carpal tunnel syndrome is the compression of the median nerve ( originated from the sixth and seventh cervical roots. Acute case of carpal tunnel syndrome are caused by hemorrhage, infection, snakebite, trauma and high pressure injection injury. Chronic cases of carpal tunnel syndrome are causes by acromegaly, amyloid, osteophytes, diabetes mellitus, birth control pills, chronic hemodialysis, hypothyroidism, compression of median nerve ( mass lesion), sarcoidosis, tuberculosis, and multiple myeloma. Other causes are hemophilia, hematoma, mucolipidosis, anomalous flexor digitorum superficialis and median nerve hamartoma. These are commonly affecting children.
References
1.Gerritsen, Annette A. M., Marc C. T. F. M. de Krom, Margaretha A. Struijs, Rob J. P. M. Scholten, Henrica C. W. de Vet, and Lex M. Bouter. “Conservative Treatment Options for Carpal Tunnel Syndrome: a Systematic Review of Randomised Controlled Trials.” Journal of Neurology 249, no. 3 (March 1, 2002): 272–280. doi:10.1007/s004150200004.
2.Gerritsen AM, de Vet HW, Scholten RM, Bertelsmann FW, de Krom MM, and Bouter LM. “Splinting Vs Surgery in the Treatment of Carpal Tunnel Syndrome: A Randomized Controlled Trial.” JAMA 288, no. 10 (September 11, 2002): 1245–1251. doi:10.1001/jama.288.10.1245.
3.Gelberman, RH, PT Hergenroeder, AR Hargens, GN Lundborg, and WH Akeson. “The Carpal Tunnel Syndrome. A Study of Carpal Canal Pressures.” The Journal of Bone & Joint Surgery 63, no. 3 (March 1, 1981): 380–383.
Treatment for carpal tunnel syndrome can be based into treatment of acute carpal tunnel syndrome and treatment of chronic carpal tunnel syndrome . Surgical decompression procedure is required in case of acute carpal tunnel syndrome while pain control and management are suitable for chronic cases of carpal tunnel syndrome.
In acute case of carpal tunnel syndrome, after making sure that the airway, breathing and circulation remain intact, the patient is refer to the hand surgeon. Hand surgeon will perform endoscopically or open surgical release of transverse carpal ligament.
In chronic case of carpal tunnel syndrome, surgical release of transverse carpal ligament may also be performed by hand surgeon open or endoscopically. Patient is advised to avoid any repetitive movement of the wrist. Visit to occupational therapist is important as nerve gliding exercises or tendon gliding exercise and ergometric testing can be performed. Local injection of corticosteroid , NASIDS or aspirin can also be given. The patient’s wrist is splint in a neutral position . The splint of the wrist is worn during night time.
Carpal tunnel syndrome can be an acute or chronic cases. Carpal tunnel syndrome may present as pain in the hand or wrist which radiates to the shoulder, elbow and forearm. The pain is exacerbated by exercise or activity which involved repetitive movement of the wrist, flexing the wrist or driving. The pain is also sever at night and relived by shaking the hand. Besides pain, patient may complain of paraesthesia, which affect the thumb, middle f, index fingers and radial aspect of the finger. Paraesthesia mostly affect the distribution of the median nerve. Loss of sensaton and loss of 2 points of discrimination may occur. Wasting and atrophy of the thenar muscle may present. Weakness of muscles are commonly affecting the opponens pollicis and abductor pollicis brevis muscles. Patient will complain of decrease fine motor control and hand dropping. Both of these muscles are innervated by median nerve.
Other tests include tourniquet test, carpal compression test and Tinel test. In tourniquet test, paraesthesia may occur after 2 minutes of inflation of the cuff to a pressure 2 mmHg above the patient systolic pressure. Tingling in the finger may occur after direct pressure is applied to the proximal part of carpal tunnel ligament in distribution of median nerve. This is known as carpal compression test. Tinel test is associated with tingling sensation after tapping the wrist over the distribution of the median nerve.
The common differential diagnosis of carpal tunnel syndrome are brachial plexitis, thoracic outlet obstruction, syringomyelia, first carpometacarpal joint osteoarthritis, cervical nerve root compression ( worst by movement of the neck or erect posture) and hand - arm vibration syndrome ( upper extremities myalgia, grip weakness, tingling and numbness when exposed to vibration and cold in the ulnar and median nerve distribution and present of Raynaud’s phenomenon.
Investigations required are analysis of rheumatoid factor, thyroid function test and immunological analysis. Fracture or arthritis degeneration in nature is detected by radiography of the wrist. Ultrasound may reveal transcarpal ligament bowing, flattening of median nerve at distal canal and swelling of the median nerve at proximal canal. MRI scan may reveal the present of fluid in the carpal tunnel, transcarpal ligament bowing, swelling of the synovium and median nerve. Carpal tunnel encroachment may be detected with CT scan. Other specific test include electromyography and nerve conduction test.
What is carpal tunnel? Carpal tunnel is an area bound by transverse carpal ligament and carpal bone. Inside carpal tunnel, there are flexor pollicis longus, median nerve, flexor digitorum profundus and flexor digitorum superficialis .
What is carpal tunnel syndrome ? Carpal tunnel syndrome is the compression of the median nerve ( originated from the sixth and seventh cervical roots. Acute case of carpal tunnel syndrome are caused by hemorrhage, infection, snakebite, trauma and high pressure injection injury. Chronic cases of carpal tunnel syndrome are causes by acromegaly, amyloid, osteophytes, diabetes mellitus, birth control pills, chronic hemodialysis, hypothyroidism, compression of median nerve ( mass lesion), sarcoidosis, tuberculosis, and multiple myeloma. Other causes are hemophilia, hematoma, mucolipidosis, anomalous flexor digitorum superficialis and median nerve hamartoma. These are commonly affecting children.
References
1.Gerritsen, Annette A. M., Marc C. T. F. M. de Krom, Margaretha A. Struijs, Rob J. P. M. Scholten, Henrica C. W. de Vet, and Lex M. Bouter. “Conservative Treatment Options for Carpal Tunnel Syndrome: a Systematic Review of Randomised Controlled Trials.” Journal of Neurology 249, no. 3 (March 1, 2002): 272–280. doi:10.1007/s004150200004.
2.Gerritsen AM, de Vet HW, Scholten RM, Bertelsmann FW, de Krom MM, and Bouter LM. “Splinting Vs Surgery in the Treatment of Carpal Tunnel Syndrome: A Randomized Controlled Trial.” JAMA 288, no. 10 (September 11, 2002): 1245–1251. doi:10.1001/jama.288.10.1245.
3.Gelberman, RH, PT Hergenroeder, AR Hargens, GN Lundborg, and WH Akeson. “The Carpal Tunnel Syndrome. A Study of Carpal Canal Pressures.” The Journal of Bone & Joint Surgery 63, no. 3 (March 1, 1981): 380–383.
