|
|
Pathology definition - Pericarditis
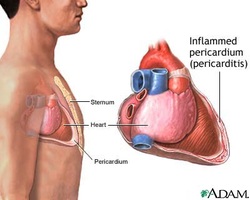
Pericarditis
There are two different forms of pericarditis. Acute pericarditis and constrictive pericarditis.
Acute pericarditis can be divided further into hemorrhagic pericarditis ( tumor), fibrinous pericarditis and suppurative pericarditis as well as serous pericarditis.
Suppurative pericarditis may present with massive inflammatory reaction on the surface of the tissue with purulent exudates. Suppurative pericarditis may occur as a result of tuberculosis, pneumococcus and staphylococcus.
Serous pericarditis may present with inflammatory reaction on the surface of the tissue with protein rich exudate. Serous pericarditis may occur as a result of renal failure, rheumatoid arthritis, viral infection, scleroderma and SLE.
Fibrinous pericarditis may present with fibrin rich exudate in pericardial space. The common causes of fibrinous pericarditis are myocardial infarction, radiation, trauma and acute renal failure.
Acute pericarditis ( hemorrhagic pericarditis, suppurative pericarditis, serous pericarditis fibrinous pericarditis ) may present with pleuritic chest pain. Pleuritic chest pain is a type of chest pain which is worsen with inspiration. Patient may also present with fever, increased jugular venous pressure during inspiration ( Kussmaul sign), cough and friction rub. Acute pericarditis is treated with corticosteroids, NSAIDS and treating the causative factors. Acute pericarditis may present with diffuse ST elevation.
Constrictive pericarditis occur as a result of progression of acute pericarditis. Constrictive pericarditis may lead to reduction in cardiac contraction and reduction in venous return. Constrictive pericarditis may present with loss of pericardial space and heart covered by fibrous scar. Constrictive pericarditis may present with symptoms and signs of right ventricular heart failure. There will be Kussmaul sign. Constrictive pericarditis is treated with pericardiectomy.
References
1.Spodick, David H. "Acute pericarditis." JAMA: the journal of the American Medical Association 289.9 (2003): 1150-1153.
2.Troughton, Richard W., Craig R. Asher, and Allan L. Klein. "Pericarditis." The Lancet 363.9410 (2004): 717-727.
There are two different forms of pericarditis. Acute pericarditis and constrictive pericarditis.
Acute pericarditis can be divided further into hemorrhagic pericarditis ( tumor), fibrinous pericarditis and suppurative pericarditis as well as serous pericarditis.
Suppurative pericarditis may present with massive inflammatory reaction on the surface of the tissue with purulent exudates. Suppurative pericarditis may occur as a result of tuberculosis, pneumococcus and staphylococcus.
Serous pericarditis may present with inflammatory reaction on the surface of the tissue with protein rich exudate. Serous pericarditis may occur as a result of renal failure, rheumatoid arthritis, viral infection, scleroderma and SLE.
Fibrinous pericarditis may present with fibrin rich exudate in pericardial space. The common causes of fibrinous pericarditis are myocardial infarction, radiation, trauma and acute renal failure.
Acute pericarditis ( hemorrhagic pericarditis, suppurative pericarditis, serous pericarditis fibrinous pericarditis ) may present with pleuritic chest pain. Pleuritic chest pain is a type of chest pain which is worsen with inspiration. Patient may also present with fever, increased jugular venous pressure during inspiration ( Kussmaul sign), cough and friction rub. Acute pericarditis is treated with corticosteroids, NSAIDS and treating the causative factors. Acute pericarditis may present with diffuse ST elevation.
Constrictive pericarditis occur as a result of progression of acute pericarditis. Constrictive pericarditis may lead to reduction in cardiac contraction and reduction in venous return. Constrictive pericarditis may present with loss of pericardial space and heart covered by fibrous scar. Constrictive pericarditis may present with symptoms and signs of right ventricular heart failure. There will be Kussmaul sign. Constrictive pericarditis is treated with pericardiectomy.
References
1.Spodick, David H. "Acute pericarditis." JAMA: the journal of the American Medical Association 289.9 (2003): 1150-1153.
2.Troughton, Richard W., Craig R. Asher, and Allan L. Klein. "Pericarditis." The Lancet 363.9410 (2004): 717-727.
