|
|
|
Emergency Strategy - How to treat cluster headache
Emergency Strategy - How to treat cluster headache
Patient will be admitted to the hospital after complaining of persistent headache unresponsive to treatment as the cause of headache is unknown. The first step in treating cluster headache include to rule out other headache related disorders which may be life threatening or just mild disorders. These includes intracerebral bleeding, trigeminal neuralgia, herpes zoster, migraine headache, intracerebral mass lesion, acute glaucoma, dental causes and meningitis as well as temporal arteritis and temporal mandibular joint syndrome.
Treatment is followed with opening of the airway, assess the breathing and consider oxygenation therapy. Supplemental oxygen may require to alleviate the symptoms. 100% of oxygen should be consider as the first step in treating cluster headache. Medication is administered. The medication include ergots, DHE, narcotic such as morphine or fentanyl, NSAIDS, prochlorperazine, somatostatin and sumatriptan.
Patient will be discharged with subcutaneous sumatriptan and oxygen therapy. Patient should present with normal neurological examination and achieve complete or moderate relief of the pain before being discharged. Verapamil is considered as prophylaxis against recurrent attacks. Follow up is important to review the patient neurological status.
Cluster headache is so severe as it may lead to suicide. Patient who suffer from cluster headache may present with one side unilateral headache which is stabbing, sharp or boring in characteristic. It will reach climax by 5 - 15 minutes. It will build it intensity and in most case is acute in term of onset. The pain from the headache will abruptly stop. The headache usually presented as pain on the temple or eye which later radiate into the jaw, cheek, ear, nose, teeth and neck. The episodes of headache typically begin at night.
The headache does not present with aura or prodrome. However it is brought by ingestion of histamine containing compound, overwork, stress, nitroglycerin, emotional experience, alcohol intake and prolonged strain.
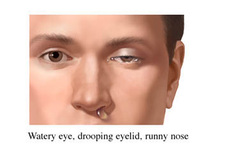
Patient typically prefer to be mobile ( move around) or stand. Patient may appear restless and agitated. Patient with cluster headache typically also present with facial flushing, sweating of forehead, sweating of face, ipsilateral headache, rhinorrhea, lacrimation, conjunctival injection, edematous eyelid, nasal congestion, miosis, ptosis and Horner syndrome.
The laboratory investigations required are full blood count ( to rule out infection), ESR ( raised ESR due to temporal arteritis), lumbar puncture( in case of subarachnoid hemorrhage or meningitis) and imaging studies ( CT scan /MRI scan- to rule out mass, tumor or hemorrhage).
The cluster headache mostly last less than an hour. Most of the headache had resolved at the time of presentation. Cluster headache is a rare condition. It is affecting men more than women. Cluster headache may last for weeks or months before remission period of 1 months. People age 20 - 40 years old are commonly affected with cluster headache. Cluster headache may occur 3 times a day at the same time of the day and mostly in fall and spring.
Cluster headache is also associated with the release of vasoactive substance from mast cell. Cluster headache may share pathological similarity with migraine. The headache /pain may follow the dermatome of the trigeminal nerve. The etiology of cluster headache is still remain unknown.
References
1.Bahra, Anish, Arne May, and Peter J. Goadsby. “Cluster Headache A Prospective Clinical Study with Diagnostic Implications.” Neurology 58, no. 3 (February 12, 2002): 354–361. doi:10.1212/WNL.58.3.354.
2.Gabai, Ivy J., and Egilius L. H. Spierings. “Prophylactic Treatment of Cluster Headache with Verapamil.” Headache: The Journal of Head and Face Pain 29, no. 3 (1989): 167–168. doi:10.1111/j.1526-4610.1989.hed2903167.x.
3.Fogan L. “Treatment of Cluster Headache: A Double-blind Comparison of Oxygen v Air Inhalation.” Archives of Neurology 42, no. 4 (April 1, 1985): 362–363. doi:10.1001/archneur.1985.04060040072015.
Patient will be admitted to the hospital after complaining of persistent headache unresponsive to treatment as the cause of headache is unknown. The first step in treating cluster headache include to rule out other headache related disorders which may be life threatening or just mild disorders. These includes intracerebral bleeding, trigeminal neuralgia, herpes zoster, migraine headache, intracerebral mass lesion, acute glaucoma, dental causes and meningitis as well as temporal arteritis and temporal mandibular joint syndrome.
Treatment is followed with opening of the airway, assess the breathing and consider oxygenation therapy. Supplemental oxygen may require to alleviate the symptoms. 100% of oxygen should be consider as the first step in treating cluster headache. Medication is administered. The medication include ergots, DHE, narcotic such as morphine or fentanyl, NSAIDS, prochlorperazine, somatostatin and sumatriptan.
Patient will be discharged with subcutaneous sumatriptan and oxygen therapy. Patient should present with normal neurological examination and achieve complete or moderate relief of the pain before being discharged. Verapamil is considered as prophylaxis against recurrent attacks. Follow up is important to review the patient neurological status.
Cluster headache is so severe as it may lead to suicide. Patient who suffer from cluster headache may present with one side unilateral headache which is stabbing, sharp or boring in characteristic. It will reach climax by 5 - 15 minutes. It will build it intensity and in most case is acute in term of onset. The pain from the headache will abruptly stop. The headache usually presented as pain on the temple or eye which later radiate into the jaw, cheek, ear, nose, teeth and neck. The episodes of headache typically begin at night.
The headache does not present with aura or prodrome. However it is brought by ingestion of histamine containing compound, overwork, stress, nitroglycerin, emotional experience, alcohol intake and prolonged strain.
Patient typically prefer to be mobile ( move around) or stand. Patient may appear restless and agitated. Patient with cluster headache typically also present with facial flushing, sweating of forehead, sweating of face, ipsilateral headache, rhinorrhea, lacrimation, conjunctival injection, edematous eyelid, nasal congestion, miosis, ptosis and Horner syndrome.
The laboratory investigations required are full blood count ( to rule out infection), ESR ( raised ESR due to temporal arteritis), lumbar puncture( in case of subarachnoid hemorrhage or meningitis) and imaging studies ( CT scan /MRI scan- to rule out mass, tumor or hemorrhage).
The cluster headache mostly last less than an hour. Most of the headache had resolved at the time of presentation. Cluster headache is a rare condition. It is affecting men more than women. Cluster headache may last for weeks or months before remission period of 1 months. People age 20 - 40 years old are commonly affected with cluster headache. Cluster headache may occur 3 times a day at the same time of the day and mostly in fall and spring.
Cluster headache is also associated with the release of vasoactive substance from mast cell. Cluster headache may share pathological similarity with migraine. The headache /pain may follow the dermatome of the trigeminal nerve. The etiology of cluster headache is still remain unknown.
References
1.Bahra, Anish, Arne May, and Peter J. Goadsby. “Cluster Headache A Prospective Clinical Study with Diagnostic Implications.” Neurology 58, no. 3 (February 12, 2002): 354–361. doi:10.1212/WNL.58.3.354.
2.Gabai, Ivy J., and Egilius L. H. Spierings. “Prophylactic Treatment of Cluster Headache with Verapamil.” Headache: The Journal of Head and Face Pain 29, no. 3 (1989): 167–168. doi:10.1111/j.1526-4610.1989.hed2903167.x.
3.Fogan L. “Treatment of Cluster Headache: A Double-blind Comparison of Oxygen v Air Inhalation.” Archives of Neurology 42, no. 4 (April 1, 1985): 362–363. doi:10.1001/archneur.1985.04060040072015.
