|
|
Pathology definition - Multiple Sclerosis
Multiple Sclerosis
Multiple sclerosis is presented as multiple firm plaques that present within the white matter of the central nervous system. This is also known as demyelination. Multiple sclerosis commonly affecting the paraventricular, brainstem and optic nerves.
The plaque consists of monocytes, gliosis, lipid laden macrophages, lymphocytes, astrocytes and depletion of oligodendrocytes.
Multiple sclerosis may be caused by genetical disorder, autoimmune disorder or environmental factors. Women are more predispose to develop multiple sclerosis as well as individual who lives in temperate climates countries. Less common in tropical countries.
Investigations required for detection of multiple sclerosis include lumbar puncture and electrophoresis. Lumbar puncture may reveal elevated IgG as well as lymphocytosis while electrophoresis may reveal the present of multiple oligoclonal bands.
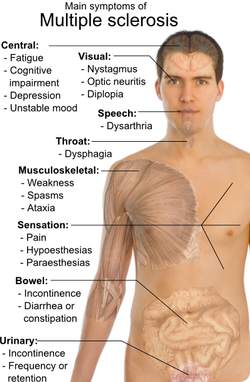
Multiple sclerosis is common in people with HLA - DR 2. Multiple sclerosis may follow a pattern of relapsing and remitting courses. The symptoms and signs are bowel incontinence and urinary incontinence due to loss of sphincter control, impairment of the sensory and motor system of the extremities and the trunk, internuclear ophthalmoplegia, ataxia, optic neuritis, nystagmus, retrobulbar neuritis and scanning speech as well as intention tremor. Besides ascending cholangitis, multiple sclerosis may also present with its own charcot triad that consists of intention tremor, nystagmus and scanning speech.
The treatment of multiple sclerosis consists of beta interferon and corticosteroid.
References
1.Putnam, Tracy J. “The Pathogenesis of Multiple Sclerosis: A Possible Vascular Factor.” New England Journal of Medicine 209, no. 16 (October 19, 1933): 786–790. doi:10.1056/NEJM193310192091604.
2.Lassmann, Hans. “Multiple Sclerosis Pathology: Evolution of Pathogenetic Concepts.” Brain Pathology 15, no. 3 (2005): 217–222. doi:10.1111/j.1750-3639.2005.tb00523.x.
Multiple sclerosis is presented as multiple firm plaques that present within the white matter of the central nervous system. This is also known as demyelination. Multiple sclerosis commonly affecting the paraventricular, brainstem and optic nerves.
The plaque consists of monocytes, gliosis, lipid laden macrophages, lymphocytes, astrocytes and depletion of oligodendrocytes.
Multiple sclerosis may be caused by genetical disorder, autoimmune disorder or environmental factors. Women are more predispose to develop multiple sclerosis as well as individual who lives in temperate climates countries. Less common in tropical countries.
Investigations required for detection of multiple sclerosis include lumbar puncture and electrophoresis. Lumbar puncture may reveal elevated IgG as well as lymphocytosis while electrophoresis may reveal the present of multiple oligoclonal bands.
Multiple sclerosis is common in people with HLA - DR 2. Multiple sclerosis may follow a pattern of relapsing and remitting courses. The symptoms and signs are bowel incontinence and urinary incontinence due to loss of sphincter control, impairment of the sensory and motor system of the extremities and the trunk, internuclear ophthalmoplegia, ataxia, optic neuritis, nystagmus, retrobulbar neuritis and scanning speech as well as intention tremor. Besides ascending cholangitis, multiple sclerosis may also present with its own charcot triad that consists of intention tremor, nystagmus and scanning speech.
The treatment of multiple sclerosis consists of beta interferon and corticosteroid.
References
1.Putnam, Tracy J. “The Pathogenesis of Multiple Sclerosis: A Possible Vascular Factor.” New England Journal of Medicine 209, no. 16 (October 19, 1933): 786–790. doi:10.1056/NEJM193310192091604.
2.Lassmann, Hans. “Multiple Sclerosis Pathology: Evolution of Pathogenetic Concepts.” Brain Pathology 15, no. 3 (2005): 217–222. doi:10.1111/j.1750-3639.2005.tb00523.x.
