|
|
Pathology definition - Multiple Myeloma
Multiple myeloma
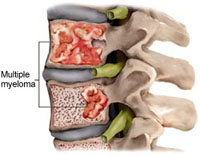
Multiple myeloma is commonly present with fried egg appearance of the neoplastic plasma cell which derived from the B lymphocytes on the bone marrow.The neoplastic cell will secretes osteoclast activating factor which later leads to lytic lesion which commonly present on the long bone. Peripheral blood smear may reveal rouleaux formation of the erythrocytes.
The neoplastic cell is originated from the proliferation of the monoclonal plasma cell. Patient with multiple myeloma may present with signs and symptoms such as fracture of the bone, bone pain, primary amyloidosis and renal insufficiency.
Multiple myeloma may present with monoclonal immunoglobulin spike M protein which is detected on the serum protein electrophoresis. Other differential diagnosis of monoclonal spike M protein is monoclonal gammopathy of undetermined significance ( MGUS) which is presented with no neoplastic infiltration of the bone marrow, no Bence Jones protein and no change in the immunoglobulin concentration. Multiple myeloma may present with detection of Bence Jones protein, in urine ( IgG light chains), increase in ESR, azotemia, hypercalcemia and hyperglobulinemia.
The lytic lesion of the long bone in patient who suffer from multiple myeloma may be detected with radiographic finding of punched out lesion. Autologous stem cell transplantation is the mode of treatment in patient who suffer from multiple myeloma.
References
1.Oshima, Kumi, Yoshinobu Kanda, Yasuhito Nannya, Makoto Kaneko, Tamae Hamaki, Miyuki Suguro, Rie Yamamoto, et al. “Clinical and Pathologic Findings in 52 Consecutively Autopsied Cases with Multiple Myeloma.” American Journal of Hematology 67, no. 1 (2001): 1–5. doi:10.1002/ajh.1067.
2.Vacca, Angelo, Domenico Ribatti, Luisa Roncali, Girolamo Ranieri, Gabriella Serio, Franco Silvestris, and Franco Dammacco. “Bone Marrow Angiogenesis and Progression in Multiple Myeloma.” British Journal of Haematology 87, no. 3 (1994): 503–508. doi:10.1111/j.1365-2141.1994.tb08304.x.
Multiple myeloma is commonly present with fried egg appearance of the neoplastic plasma cell which derived from the B lymphocytes on the bone marrow.The neoplastic cell will secretes osteoclast activating factor which later leads to lytic lesion which commonly present on the long bone. Peripheral blood smear may reveal rouleaux formation of the erythrocytes.
The neoplastic cell is originated from the proliferation of the monoclonal plasma cell. Patient with multiple myeloma may present with signs and symptoms such as fracture of the bone, bone pain, primary amyloidosis and renal insufficiency.
Multiple myeloma may present with monoclonal immunoglobulin spike M protein which is detected on the serum protein electrophoresis. Other differential diagnosis of monoclonal spike M protein is monoclonal gammopathy of undetermined significance ( MGUS) which is presented with no neoplastic infiltration of the bone marrow, no Bence Jones protein and no change in the immunoglobulin concentration. Multiple myeloma may present with detection of Bence Jones protein, in urine ( IgG light chains), increase in ESR, azotemia, hypercalcemia and hyperglobulinemia.
The lytic lesion of the long bone in patient who suffer from multiple myeloma may be detected with radiographic finding of punched out lesion. Autologous stem cell transplantation is the mode of treatment in patient who suffer from multiple myeloma.
References
1.Oshima, Kumi, Yoshinobu Kanda, Yasuhito Nannya, Makoto Kaneko, Tamae Hamaki, Miyuki Suguro, Rie Yamamoto, et al. “Clinical and Pathologic Findings in 52 Consecutively Autopsied Cases with Multiple Myeloma.” American Journal of Hematology 67, no. 1 (2001): 1–5. doi:10.1002/ajh.1067.
2.Vacca, Angelo, Domenico Ribatti, Luisa Roncali, Girolamo Ranieri, Gabriella Serio, Franco Silvestris, and Franco Dammacco. “Bone Marrow Angiogenesis and Progression in Multiple Myeloma.” British Journal of Haematology 87, no. 3 (1994): 503–508. doi:10.1111/j.1365-2141.1994.tb08304.x.
