Symptom finder - The causes of cough

Symptom finder - The causes of cough
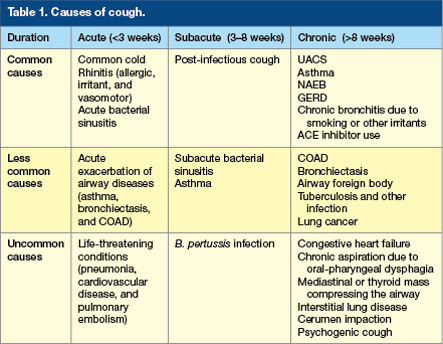
Cough is divided into acute cough and chronic cough. Acute cough is caused by respiratory tract infection and inhaled foreign bodies ( chronic cough is caused by sarcoidosis, drug ( ACE inhibitor), gastro esophageal reflux , post nasal drip and asthma ( chronic non productive cough) and blood stained pulmonary embolism, lung cancer blood stained, pink frothy sputum pulmonary edema, purulent sputum bronchiectasis, TB and mucosa /purulent sputum CPOD for chronic productive cough.
Cough is useful in removal of foreign particles and secretion from the lung by preventing aspiration due to the cough reflex explosive expiration.
Cough may be acute or chronic in nature. Chronic cough is a cough which persists for more than 3 weeks. Inhalation of foreign body may lead to unrelenting bout of cough which is violent in nature. This may lead to cyanosis and loss of consciousness . Life saving cricothyroidotomy is required.
The differential diagnosis of coughing an also be determine by the quantity, appearance and frequency of the sputum expectorated. Bronchiectasis and chronic bronchitis are considered by the production of purulent sputum. Tuberculosis, pulmonary embolism and bronchogenic carcinoma may occur with expectoration of the blood stained sputum.
There are two form of wheeze. This include monophonic wheeze due to tumor or intraluminal obstruction of foreign bodies and seasonal or episodic wheezing due to asthma which is also accompanied with shortness of breath at night. Coughing that present with sudden onset of shortness of breath/dyspnea may occur due to pulmonary embolism or aspiration. Pulmonary edema is suggestive of shortness of breath /dyspnea which is worst on recumbency. Lung tumor and tuberculosis are common with weight loss, Chest pain unrelenting in nature is suggestive of bony metastasis from bronchogenic carcinoma /lung tumor. Pneumonia and pulmonary emboli are associated with pleuritic chest pain. Gastroesophageal disease is present with coughing and retrosternal burning pain in the chest precipitated by posture. Post nasal drip may occur due to rhinitis as a result of frequent throat clearing due to nasal discharge or history of allergy. Pneumonia and pulmonary emboli may present with chest pain which is pleuritic in nature.
Smoker may suffer from coughing due to smoking alone or chronic bronchitis or bronchogenic carcinoma in case of prolonged smoking. Smoker may also present with hoarseness of voice. History of foreign travel to tuberculosis endemic area are also vital.
On examination, raised temperature/pyrexia is an indication of pulmonary embolism or infectious causes. Barrel shaped is associated with COPD. Cachectic is common in patient with TB and lung cancer. COPD and pulmonary embolism may present with cyanosis. Bronchial carcinoma as well as bronchiectasis patient may present with clubbing of the finger. Raised JVP is associated with congestive cardiac failure while palpable supraclavicular node is common in lung cancer, tuberculosis and respiratory tract infection.Dullness to percussion, decrease vocal resonance and absent of breath sound are signs of pleural effusion which is a manifestation of bronchial carcinoma besides segmental collapse of lung. Coarse crepitations are common feature of pulmonary edema or bronchiectasis. Wheeze which is widespread is characteristic of asthma. Bronchial luminal obstruction may present with fixed inspiratory wheeze.
Cough is divided into acute cough and chronic cough. Acute cough is caused by respiratory tract infection and inhaled foreign bodies ( chronic cough is caused by sarcoidosis, drug ( ACE inhibitor), gastro esophageal reflux , post nasal drip and asthma ( chronic non productive cough) and blood stained pulmonary embolism, lung cancer blood stained, pink frothy sputum pulmonary edema, purulent sputum bronchiectasis, TB and mucosa /purulent sputum CPOD for chronic productive cough.
Cough is useful in removal of foreign particles and secretion from the lung by preventing aspiration due to the cough reflex explosive expiration.
Cough may be acute or chronic in nature. Chronic cough is a cough which persists for more than 3 weeks. Inhalation of foreign body may lead to unrelenting bout of cough which is violent in nature. This may lead to cyanosis and loss of consciousness . Life saving cricothyroidotomy is required.
The differential diagnosis of coughing an also be determine by the quantity, appearance and frequency of the sputum expectorated. Bronchiectasis and chronic bronchitis are considered by the production of purulent sputum. Tuberculosis, pulmonary embolism and bronchogenic carcinoma may occur with expectoration of the blood stained sputum.
There are two form of wheeze. This include monophonic wheeze due to tumor or intraluminal obstruction of foreign bodies and seasonal or episodic wheezing due to asthma which is also accompanied with shortness of breath at night. Coughing that present with sudden onset of shortness of breath/dyspnea may occur due to pulmonary embolism or aspiration. Pulmonary edema is suggestive of shortness of breath /dyspnea which is worst on recumbency. Lung tumor and tuberculosis are common with weight loss, Chest pain unrelenting in nature is suggestive of bony metastasis from bronchogenic carcinoma /lung tumor. Pneumonia and pulmonary emboli are associated with pleuritic chest pain. Gastroesophageal disease is present with coughing and retrosternal burning pain in the chest precipitated by posture. Post nasal drip may occur due to rhinitis as a result of frequent throat clearing due to nasal discharge or history of allergy. Pneumonia and pulmonary emboli may present with chest pain which is pleuritic in nature.
Smoker may suffer from coughing due to smoking alone or chronic bronchitis or bronchogenic carcinoma in case of prolonged smoking. Smoker may also present with hoarseness of voice. History of foreign travel to tuberculosis endemic area are also vital.
On examination, raised temperature/pyrexia is an indication of pulmonary embolism or infectious causes. Barrel shaped is associated with COPD. Cachectic is common in patient with TB and lung cancer. COPD and pulmonary embolism may present with cyanosis. Bronchial carcinoma as well as bronchiectasis patient may present with clubbing of the finger. Raised JVP is associated with congestive cardiac failure while palpable supraclavicular node is common in lung cancer, tuberculosis and respiratory tract infection.Dullness to percussion, decrease vocal resonance and absent of breath sound are signs of pleural effusion which is a manifestation of bronchial carcinoma besides segmental collapse of lung. Coarse crepitations are common feature of pulmonary edema or bronchiectasis. Wheeze which is widespread is characteristic of asthma. Bronchial luminal obstruction may present with fixed inspiratory wheeze.
The laboratory investigations are just full blood count, sputum culture, peak flow, respiratory function tests, chest x ray, pulmonary angiography, V/Q scan, CT thorax and pH studies.
In full blood count investigations, raised white cell count is an indication of pulmonary embolism and infection. Sputum culture is considered as in case of productive cough to rule out tuberculosis with Ziehl - Neelsen staining. Peak flow / peak expiratory flow is useful in assessing the present of asthma ( which indicates low peak volume). Formal respiratory function test is useful for diagnosing any obstruction of the airway ( bronchiectasis, chronic bronchitis or asthma ). FIxed airway obstruction is determined by flow volume loops.
Chest X ray may reveal the present of bronchiectasis with the finding of the dilated bronchi and persistent area of infection. Area of consolidation may reveal infection ( pneumonia). TB is characterized with calcification, apical pulmonary consolidation and hilar lymphadenopathy. Pulmonary edema is characterized by radiological features of cardiac failure such as kerley B line ( horizontal lines 1-2 cm in the peripheral of the lung ), pleural effusion bilaterally, upper lobe diversion of pulmonary vein, bilateral patchy shadowing and cardiomegaly. Bronchogenic carcinoma may present as peripheral mass, hilar mass, consolidation or collapse of the lung due to airway obstruction. Sarcoidosis is suggestive of bilateral hilar lymphadenopathy.
Pulmonary angiography is considered in suspected case of pulmonary embolism and decision need to be made to thrombolysis or perform surgical procedure. V/Q scan is considered when pulmonary embolism is suspected. Staging and diagnosing of bronchiectasis can be obtained with CT scan of the thorax. 24 hour pH is useful in diagnosing gastro- esophageal reflux disease.
In full blood count investigations, raised white cell count is an indication of pulmonary embolism and infection. Sputum culture is considered as in case of productive cough to rule out tuberculosis with Ziehl - Neelsen staining. Peak flow / peak expiratory flow is useful in assessing the present of asthma ( which indicates low peak volume). Formal respiratory function test is useful for diagnosing any obstruction of the airway ( bronchiectasis, chronic bronchitis or asthma ). FIxed airway obstruction is determined by flow volume loops.
Chest X ray may reveal the present of bronchiectasis with the finding of the dilated bronchi and persistent area of infection. Area of consolidation may reveal infection ( pneumonia). TB is characterized with calcification, apical pulmonary consolidation and hilar lymphadenopathy. Pulmonary edema is characterized by radiological features of cardiac failure such as kerley B line ( horizontal lines 1-2 cm in the peripheral of the lung ), pleural effusion bilaterally, upper lobe diversion of pulmonary vein, bilateral patchy shadowing and cardiomegaly. Bronchogenic carcinoma may present as peripheral mass, hilar mass, consolidation or collapse of the lung due to airway obstruction. Sarcoidosis is suggestive of bilateral hilar lymphadenopathy.
Pulmonary angiography is considered in suspected case of pulmonary embolism and decision need to be made to thrombolysis or perform surgical procedure. V/Q scan is considered when pulmonary embolism is suspected. Staging and diagnosing of bronchiectasis can be obtained with CT scan of the thorax. 24 hour pH is useful in diagnosing gastro- esophageal reflux disease.
