Acute Bronchitis Symptoms
Acute Bronchitis
Acute bronchitis is also known as cold chest.
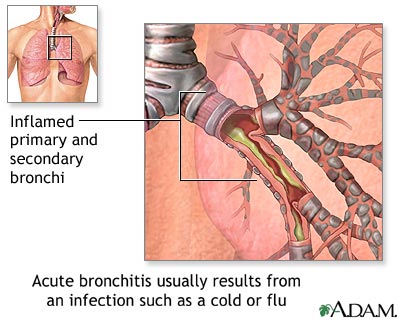
Acute bronchitis is the inflammation of trachea and bronchi.
Viral infections are the leading cause of bronchitis (rhinovirus, influenza virus, adenovirus,
respiratory syncytial virus). Other causes include atypical organisms (Mycoplasma, Chlamydia pneumoniae) and bacterial infections (Haemophilus influenzae, Moraxella, Streptococcus pneumoniae).
Symptoms and signs of acute bronchitis are cough, usually worse in the morning, often productive; mainly caused by transient bronchial hyperresponsiveness, low-grade fever, substernal discomfort worsened by coughing, postnasal drip, pharyngeal injection, rhonchi that may clear after cough and occasional wheezing.
Differential diagnosis of acute bronchitis are aspiration,cystic fibrosis, pharyngitis,cough secondary to medications,neoplasm (elderly patients), influenza, allergic aspergillosis gastroesophageal reflux disease,congestive heart failure (in elderly patients),bronchogenic neoplasm,asthma, pneumonia and asthma.
Chest x-ray examination is usually reserved for patients with suspected pneumonia, influenza, or underlying chronic obstructive pulmonary disease (COPD) and no improvement with therapy.
There are different forms of treatment for acute bronchitis. Inhaled bronchodilators (e.g., albuterol,metaproterenol) prn for 1 to 2 wk in patients with wheezing or troublesome cough. Inhaled albuterol has been proven effective in reducing the duration of cough in adults with uncomplicated acute bronchitis.
Cough suppression with dextromethorphan and guaifenesin is commonly recommended; addition of codeine for cough suppression if cough is severe and is significantly interrupting patient’s sleep pattern.
Use of antibiotics (TMP-SMX, amoxicillin, doxycycline, cefuroxime) for acute bronchitisis generally not indicated; should be considered only in patients with concomitant COPD and purulent sputum or in patients unresponsive to prolonged conservative treatment.
Antibiotics are overused in patients with acute bronchitis (70% to 90% of office visits for acute bronchitis result in treatment with antibiotics); this practice pattern is contributing to increases in resistant organisms.
The supportive and preventive measure may include avoidance of tobacco and other pulmonary irritants,increased fluid intake and use of vaporizer to increase room humidity
Acute bronchitis is also known as cold chest.
Acute bronchitis is the inflammation of trachea and bronchi.
Viral infections are the leading cause of bronchitis (rhinovirus, influenza virus, adenovirus,
respiratory syncytial virus). Other causes include atypical organisms (Mycoplasma, Chlamydia pneumoniae) and bacterial infections (Haemophilus influenzae, Moraxella, Streptococcus pneumoniae).
Symptoms and signs of acute bronchitis are cough, usually worse in the morning, often productive; mainly caused by transient bronchial hyperresponsiveness, low-grade fever, substernal discomfort worsened by coughing, postnasal drip, pharyngeal injection, rhonchi that may clear after cough and occasional wheezing.
Differential diagnosis of acute bronchitis are aspiration,cystic fibrosis, pharyngitis,cough secondary to medications,neoplasm (elderly patients), influenza, allergic aspergillosis gastroesophageal reflux disease,congestive heart failure (in elderly patients),bronchogenic neoplasm,asthma, pneumonia and asthma.
Chest x-ray examination is usually reserved for patients with suspected pneumonia, influenza, or underlying chronic obstructive pulmonary disease (COPD) and no improvement with therapy.
There are different forms of treatment for acute bronchitis. Inhaled bronchodilators (e.g., albuterol,metaproterenol) prn for 1 to 2 wk in patients with wheezing or troublesome cough. Inhaled albuterol has been proven effective in reducing the duration of cough in adults with uncomplicated acute bronchitis.
Cough suppression with dextromethorphan and guaifenesin is commonly recommended; addition of codeine for cough suppression if cough is severe and is significantly interrupting patient’s sleep pattern.
Use of antibiotics (TMP-SMX, amoxicillin, doxycycline, cefuroxime) for acute bronchitisis generally not indicated; should be considered only in patients with concomitant COPD and purulent sputum or in patients unresponsive to prolonged conservative treatment.
Antibiotics are overused in patients with acute bronchitis (70% to 90% of office visits for acute bronchitis result in treatment with antibiotics); this practice pattern is contributing to increases in resistant organisms.
The supportive and preventive measure may include avoidance of tobacco and other pulmonary irritants,increased fluid intake and use of vaporizer to increase room humidity