|
|
Pathology definition - Cardiomyopathy
Cardiomyopathy
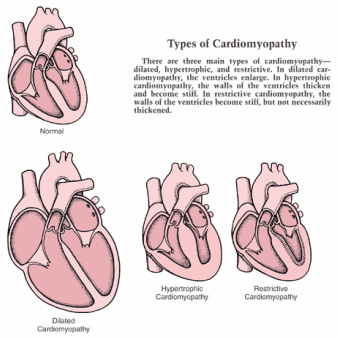
There are three different forms of cardiomyopathy. These are dilated cardiomyopathy, hypertrophic cardiomyopathy and restrictive cardiomyopathy.
Dilated cardiomyopathy is associated with congestive heart failure. Dilated cardiomyopathy is treated with anticoagulant and ACE inhibitor. Dilated cardiomyopathy is the most common form of cardiomyopathy. It is presented with dilation of all the chambers of the heart with interstitial fibrosis and muscle cells hypertrophy. Dilated cardiomyopathy occur due to cocaine abuse, muscular dystrophy, post myocarditis, alcoholism, vitamin B1 deficiency ( wet beriberi) and doxorubicin toxicity. Dilated cardiomyopathy will lead to systolic dysfunction and balloon heart images on the chest x ray.
Hypertrophic cardiomyopathy may present with hypertrophy of the myocardium and hypertrophy of the interventricular septum. There will be reduction in cardiac output due to decreased in diastolic filling and obstruction of the left ventricular outflow tract. Hypertrophic cardiomyopathy may present with palpitation, angina, syncope, dyspnea and sudden death. Hypertrophic cardiomyopathy occurs due to autosomal dominant mutation in beta myosin heavy chain gene.Hypertrophic cardiomyopathy is treated with beta blocker.
Restrictive cardiomyopathy may present with dyspnea, edema and weakness. Restrictive cardiomyopathy is presented with interstitial fibrosis which lead to reduction in cardiac output as a result do decreased in diastolic filling and decreased in ventricular compliance. Restrictive cardiomyopathy may be cause by amyloidosis, endocardial fibroelastosis, endomyocardial fibrosis, sarcoidosis, and systemic sclerosis.
References
1.Maron, Barry J. "Hypertrophic cardiomyopathy." JAMA: the journal of the American Medical Association 287.10 (2002): 1308-1320.
2.Rihal, Charanjit S., et al. "Systolic and diastolic dysfunction in patients with clinical diagnosis of dilated cardiomyopathy. Relation to symptoms and prognosis." Circulation 90.6 (1994): 2772-2779.
3.Benotti, JOSEPH R., W. I. L. L. I. A. M. Grossman, and PETER F. Cohn. "Clinical profile of restrictive cardiomyopathy." Circulation 61.6 (1980): 1206-1212.
There are three different forms of cardiomyopathy. These are dilated cardiomyopathy, hypertrophic cardiomyopathy and restrictive cardiomyopathy.
Dilated cardiomyopathy is associated with congestive heart failure. Dilated cardiomyopathy is treated with anticoagulant and ACE inhibitor. Dilated cardiomyopathy is the most common form of cardiomyopathy. It is presented with dilation of all the chambers of the heart with interstitial fibrosis and muscle cells hypertrophy. Dilated cardiomyopathy occur due to cocaine abuse, muscular dystrophy, post myocarditis, alcoholism, vitamin B1 deficiency ( wet beriberi) and doxorubicin toxicity. Dilated cardiomyopathy will lead to systolic dysfunction and balloon heart images on the chest x ray.
Hypertrophic cardiomyopathy may present with hypertrophy of the myocardium and hypertrophy of the interventricular septum. There will be reduction in cardiac output due to decreased in diastolic filling and obstruction of the left ventricular outflow tract. Hypertrophic cardiomyopathy may present with palpitation, angina, syncope, dyspnea and sudden death. Hypertrophic cardiomyopathy occurs due to autosomal dominant mutation in beta myosin heavy chain gene.Hypertrophic cardiomyopathy is treated with beta blocker.
Restrictive cardiomyopathy may present with dyspnea, edema and weakness. Restrictive cardiomyopathy is presented with interstitial fibrosis which lead to reduction in cardiac output as a result do decreased in diastolic filling and decreased in ventricular compliance. Restrictive cardiomyopathy may be cause by amyloidosis, endocardial fibroelastosis, endomyocardial fibrosis, sarcoidosis, and systemic sclerosis.
References
1.Maron, Barry J. "Hypertrophic cardiomyopathy." JAMA: the journal of the American Medical Association 287.10 (2002): 1308-1320.
2.Rihal, Charanjit S., et al. "Systolic and diastolic dysfunction in patients with clinical diagnosis of dilated cardiomyopathy. Relation to symptoms and prognosis." Circulation 90.6 (1994): 2772-2779.
3.Benotti, JOSEPH R., W. I. L. L. I. A. M. Grossman, and PETER F. Cohn. "Clinical profile of restrictive cardiomyopathy." Circulation 61.6 (1980): 1206-1212.
