Barotitis
Barotitis is associated with trauma/barotrauma of the inner and middle ear. The barotrauma may be caused by flying and scuba diving.
In scuba diving, barotitis, is avoided if gradual descent and ascent are taken. This maneuver will reduce the risk of developing barotrauma. The preventive measure such as performing valsalva maneuver; intake of decongestant and anti histamine is particularly helpful in preventing barotitis. Not all form of flying is causing barotitis. People who travel with commercial airlines are unlikely to develop severe barotitis. (Development of the mild negative pressure is common in the middle ear after flying.) Significant barotrauma which later lead to barotitis are common with military aircraft flyers or scuba divers because of the rapid changes in the altitude.
The incidence of the developing barotitis, after a single flight is 20% in adult and 8-55% for children. The risks of developing barotitis are eustachian tube dysfunction, viral upper respiratory infection, and allergic rhinitis.
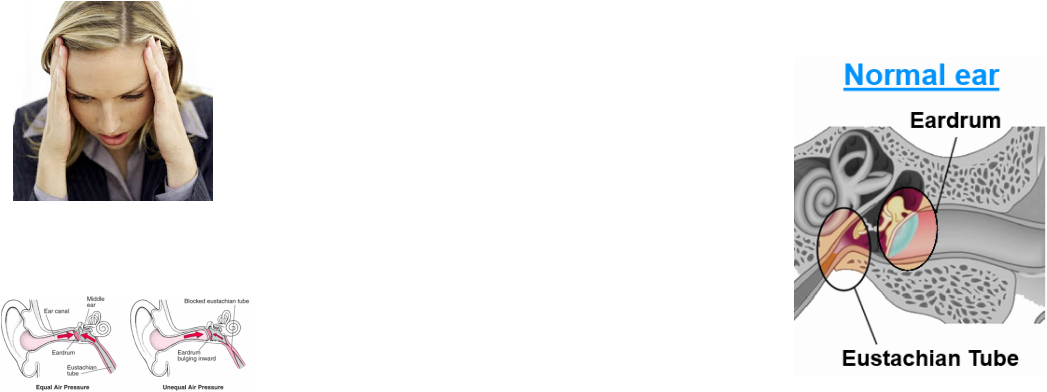
In term of pathophysiology, the eustachian tube and parts of the ear (outer, middle and inner ears play a major part. While the plane is ascending, the ambient pressure will decrease. The excess middle ear pressure will vent by the eustachian tube while tympanic membrane bulged outward. The pressure is finally equalized. Barotitis is not developing.
While the airplane is descending or during scuba diving, the ambient pressure will increase. This will cause the tympanic membrane to bulge inward and eustachian tube to resists the flow of inward air to the middle ear. Equalization of the pressure is difficult although the eustachian tube is functioning properly.
Barotrauma of the inner ear may lead to rupture of the window of the labyrinthine. Formation of exudate, bleeding and vascular engorgement may occur because of barotitis /barotrauma.
When the ambient pressure is greater than the pressure in the middle ear (differential pressure of greater than 60mmHg), the person may report of subjective discomfort. If the differential in pressure is more than 90mmHg, the eustachian tube will fall into the state of “ locked”. This is caused by palatal musculature weakness to open the eustachian tube. The equalization of the pressure cannot be achieved because of impairment of the flow of air. If the differences of the ambient pressure and middle ear pressure us greater than 100 - 500 mmHg, the tympanic membrane will rupture. Barotitis is also associated with nasal congestion.
Significant injury and symptoms of the disease are less common in commercial airlines. However, mild negative pressure in the middle ear is still common. Scuba diver or military aircraft pilot may suffer from significant symptoms and injury.
The complications of barotitis are the rupture of the tympanic membrane, rupture of the round or oval window, loss of hearing and vertigo as well as hemorrhage.
In mild cases, there should be a spontaneous complete remission. Tympanostomy and tympanotomy area rarely required to relieve the pain as well as the pressure and the complication. The variable result is associated with inner ear injuries owed to barotitis in term of vestibular and auditory symptoms.
The differential diagnoses of barotitis are trauma such as exposure to loud noise or blunt trauma of the tympanic membrane and infection such as acute otitis media or otitis media with effusion.
The patient who presented with barotrauma /barotitis will complain of decreased in hearing, pressure sensation and pain in the ear. Patient with damage to the inner ear may complain of auditory and vestibular symptoms. Important questions to ask the patient are “ has the patient being slapped in the ear by a child?”, “has the patient attend any heavy metal concert?” “ Has the patient inserted a foreign bodies ( Q- Tip cotton swab) into the ear?” or “has the patient travel by plane recently or is the patient a scuba diver?”
Physical examination should focus on Teed’s classification. Grade 0 indicates normal appearance of the tympanic membrane. Grade 1 indicates redness and retraction in the Shrapnell membrane as well as along the manubrium. Grade 32 indicates redness of the entire eardrum as well as the retraction of the eardrum. Grade 3 is a combination of the present of hemotympanum, clear exudate, redness and retraction of the entire eardrum. Tympanic membrane which is perforated is an indication of Grade 4 of Teed’s classification . The patient is also assessed for any evidence of hearing loss and nystagmus. Patients who are symptomatic but with normal physical examination or patient with signs of barotrauma may require hearing test. MRI is important to rule out any damage to the inner ear and should be considered in patient with vestibular symptoms.
Therapy may include tympanostomy, tympanotomy, Otovent, Politzer bag, chewing, swallowing, yawning, and valsalva maneuver as well as medication.
Tympanostomy and tympanotomy are considered in severe cases. Otovent or Politzer bag may equalize the pressure. Otovent is used as an instrument of prevention mostly in children ages 2- 6 years old. Politzer is useful as secondary therapy if valsalva maneuver or decongestant unable to improve the disequilibrium of the pressure. Chewing, swallowing, yawning is considered while the scuba diver is ascending to the water surface or while the airplane is ascending on the air. Chewing, swallowing and yawning will lead to the release of pressure from the eustachian tube.
Pinching the nostril closed and blowing the nose is helpful to force air into the middle ear while descending or diving. This action is called valsalva maneuver and it is useful to equalize the pressure between the middle ear and the environment.
Otorhinolaryngologist may perform myringomyotomy in patient with persistent eustachian tube dysfunction or suffer from excruciating pain.
Decongestant and antihistamine are the form of medication required to treat barotitis. Decongestant may constrict the mucosal arterioles to enhanced the function of eustachian tube . Nasal decongestant is used 1 hour prior to diving /travel by airplane and 1/2 hour prior to descent of the plane. Oral decongestant is given 1-2 days prior to scuba diving /travel.
Antihistamine is useful to enhance the orifices of the eustachian tube and reducing the edema of the mucosal. Anti - histamine is considered in a day expected for the pressure changed.
The differences in pressure will take a few days for it to be resolved and return to the normal atmosphere pressure. ( Without any evidence of damage of the middle ear)
There is a variable rate of improvement for barotitis that occurs because of middle and inner ear injuries. Some injuries may be reversible / temporary such as damage to the tympanic membrane. Some injuries may be permanent owed to injury to the organ of Corti.
It is wise for scuba diver to ascent and descent gradually. Valsalva maneuver, decongestants and antihistamines are useful as preventive measures. The mother is also advised to nurse the child, have the child to eat or take a bottle during the ascent and descent. This activity will increase the movement of the pharyngeal that will open the eustachian tube repeatedly and equalize the environmental pressure and middle ear pressure. The use of the decongestant is useful if prior to the flight especially if the child suffer from upper respiratory tract infection. The pressure of otitis media with the effusion is protective against barotitis.
Barotitis is associated with trauma/barotrauma of the inner and middle ear. The barotrauma may be caused by flying and scuba diving.
In scuba diving, barotitis, is avoided if gradual descent and ascent are taken. This maneuver will reduce the risk of developing barotrauma. The preventive measure such as performing valsalva maneuver; intake of decongestant and anti histamine is particularly helpful in preventing barotitis. Not all form of flying is causing barotitis. People who travel with commercial airlines are unlikely to develop severe barotitis. (Development of the mild negative pressure is common in the middle ear after flying.) Significant barotrauma which later lead to barotitis are common with military aircraft flyers or scuba divers because of the rapid changes in the altitude.
The incidence of the developing barotitis, after a single flight is 20% in adult and 8-55% for children. The risks of developing barotitis are eustachian tube dysfunction, viral upper respiratory infection, and allergic rhinitis.
In term of pathophysiology, the eustachian tube and parts of the ear (outer, middle and inner ears play a major part. While the plane is ascending, the ambient pressure will decrease. The excess middle ear pressure will vent by the eustachian tube while tympanic membrane bulged outward. The pressure is finally equalized. Barotitis is not developing.
While the airplane is descending or during scuba diving, the ambient pressure will increase. This will cause the tympanic membrane to bulge inward and eustachian tube to resists the flow of inward air to the middle ear. Equalization of the pressure is difficult although the eustachian tube is functioning properly.
Barotrauma of the inner ear may lead to rupture of the window of the labyrinthine. Formation of exudate, bleeding and vascular engorgement may occur because of barotitis /barotrauma.
When the ambient pressure is greater than the pressure in the middle ear (differential pressure of greater than 60mmHg), the person may report of subjective discomfort. If the differential in pressure is more than 90mmHg, the eustachian tube will fall into the state of “ locked”. This is caused by palatal musculature weakness to open the eustachian tube. The equalization of the pressure cannot be achieved because of impairment of the flow of air. If the differences of the ambient pressure and middle ear pressure us greater than 100 - 500 mmHg, the tympanic membrane will rupture. Barotitis is also associated with nasal congestion.
Significant injury and symptoms of the disease are less common in commercial airlines. However, mild negative pressure in the middle ear is still common. Scuba diver or military aircraft pilot may suffer from significant symptoms and injury.
The complications of barotitis are the rupture of the tympanic membrane, rupture of the round or oval window, loss of hearing and vertigo as well as hemorrhage.
In mild cases, there should be a spontaneous complete remission. Tympanostomy and tympanotomy area rarely required to relieve the pain as well as the pressure and the complication. The variable result is associated with inner ear injuries owed to barotitis in term of vestibular and auditory symptoms.
The differential diagnoses of barotitis are trauma such as exposure to loud noise or blunt trauma of the tympanic membrane and infection such as acute otitis media or otitis media with effusion.
The patient who presented with barotrauma /barotitis will complain of decreased in hearing, pressure sensation and pain in the ear. Patient with damage to the inner ear may complain of auditory and vestibular symptoms. Important questions to ask the patient are “ has the patient being slapped in the ear by a child?”, “has the patient attend any heavy metal concert?” “ Has the patient inserted a foreign bodies ( Q- Tip cotton swab) into the ear?” or “has the patient travel by plane recently or is the patient a scuba diver?”
Physical examination should focus on Teed’s classification. Grade 0 indicates normal appearance of the tympanic membrane. Grade 1 indicates redness and retraction in the Shrapnell membrane as well as along the manubrium. Grade 32 indicates redness of the entire eardrum as well as the retraction of the eardrum. Grade 3 is a combination of the present of hemotympanum, clear exudate, redness and retraction of the entire eardrum. Tympanic membrane which is perforated is an indication of Grade 4 of Teed’s classification . The patient is also assessed for any evidence of hearing loss and nystagmus. Patients who are symptomatic but with normal physical examination or patient with signs of barotrauma may require hearing test. MRI is important to rule out any damage to the inner ear and should be considered in patient with vestibular symptoms.
Therapy may include tympanostomy, tympanotomy, Otovent, Politzer bag, chewing, swallowing, yawning, and valsalva maneuver as well as medication.
Tympanostomy and tympanotomy are considered in severe cases. Otovent or Politzer bag may equalize the pressure. Otovent is used as an instrument of prevention mostly in children ages 2- 6 years old. Politzer is useful as secondary therapy if valsalva maneuver or decongestant unable to improve the disequilibrium of the pressure. Chewing, swallowing, yawning is considered while the scuba diver is ascending to the water surface or while the airplane is ascending on the air. Chewing, swallowing and yawning will lead to the release of pressure from the eustachian tube.
Pinching the nostril closed and blowing the nose is helpful to force air into the middle ear while descending or diving. This action is called valsalva maneuver and it is useful to equalize the pressure between the middle ear and the environment.
Otorhinolaryngologist may perform myringomyotomy in patient with persistent eustachian tube dysfunction or suffer from excruciating pain.
Decongestant and antihistamine are the form of medication required to treat barotitis. Decongestant may constrict the mucosal arterioles to enhanced the function of eustachian tube . Nasal decongestant is used 1 hour prior to diving /travel by airplane and 1/2 hour prior to descent of the plane. Oral decongestant is given 1-2 days prior to scuba diving /travel.
Antihistamine is useful to enhance the orifices of the eustachian tube and reducing the edema of the mucosal. Anti - histamine is considered in a day expected for the pressure changed.
The differences in pressure will take a few days for it to be resolved and return to the normal atmosphere pressure. ( Without any evidence of damage of the middle ear)
There is a variable rate of improvement for barotitis that occurs because of middle and inner ear injuries. Some injuries may be reversible / temporary such as damage to the tympanic membrane. Some injuries may be permanent owed to injury to the organ of Corti.
It is wise for scuba diver to ascent and descent gradually. Valsalva maneuver, decongestants and antihistamines are useful as preventive measures. The mother is also advised to nurse the child, have the child to eat or take a bottle during the ascent and descent. This activity will increase the movement of the pharyngeal that will open the eustachian tube repeatedly and equalize the environmental pressure and middle ear pressure. The use of the decongestant is useful if prior to the flight especially if the child suffer from upper respiratory tract infection. The pressure of otitis media with the effusion is protective against barotitis.
