Pathology definition - Emphysema
Emphysema
Emphysema is part of chronic obstructive pulmonary disease. Patient may present with prominent physical symptoms and signs such as dyspnea, shortness of breath, cyanosis, tachycardia, pink puffers ( forced expiration through the pursed lip) , barrel shaped chest and accessory respiratory muscle used.
Emphysema may occur due to deficiency of the alpha 1 antitrypsin ( hereditary condition) and smoking.Smoking will inactivate the action of alpha 1 anti trypsin which is protective in nature and attract neutrophils. There will be decreased in the FEV1/ FVC ratio, ( FEV1= forced expiratory volume in 1 second and FVC = forced vital capacity). There will also be increase in the total lung capacity and residual volumes.
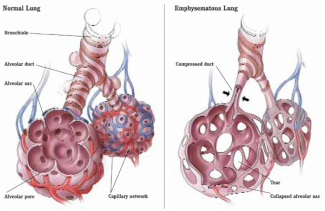
Pathologically, there will be destruction of the alveolar walls with enlargement of the air spaces. The destruction of the alveolar wall is caused by enzyme elastase which digest elastin component of the alveolar wall. The enzyme elastase will be inactivated by alpha 1 anti trypsin.
There are four patterns of emphysema. These are centri acinar emphysema which lead to dilation of the respiratory bronchioles mostly in the upper lobes of the lung. Centriacinar emphysema mostly seen in smokers. The next pattern is irregular emphysema which involved the distal alveoli. The distal alveoli will be dilated and presented with large blebs. Pan acinar emphysema mostly due to deficiency of the alpha 1 anti trypsin and involve the dilation of the entire acinus. Irregular emphysema is most commonly occur with irregular involvement of the acinus which is scared and inflamed. Chest x ray may reveal flattened diaphragm and hyperinflation of the chest with bullae.
Patient is treated with bronchodilators, oxyygen and advice on smoking cessation. The complication of emphysema may include pneumothorax, respiratory failure and cor pulmonale.
Emphysema is part of chronic obstructive pulmonary disease. Patient may present with prominent physical symptoms and signs such as dyspnea, shortness of breath, cyanosis, tachycardia, pink puffers ( forced expiration through the pursed lip) , barrel shaped chest and accessory respiratory muscle used.
Emphysema may occur due to deficiency of the alpha 1 antitrypsin ( hereditary condition) and smoking.Smoking will inactivate the action of alpha 1 anti trypsin which is protective in nature and attract neutrophils. There will be decreased in the FEV1/ FVC ratio, ( FEV1= forced expiratory volume in 1 second and FVC = forced vital capacity). There will also be increase in the total lung capacity and residual volumes.
Pathologically, there will be destruction of the alveolar walls with enlargement of the air spaces. The destruction of the alveolar wall is caused by enzyme elastase which digest elastin component of the alveolar wall. The enzyme elastase will be inactivated by alpha 1 anti trypsin.
There are four patterns of emphysema. These are centri acinar emphysema which lead to dilation of the respiratory bronchioles mostly in the upper lobes of the lung. Centriacinar emphysema mostly seen in smokers. The next pattern is irregular emphysema which involved the distal alveoli. The distal alveoli will be dilated and presented with large blebs. Pan acinar emphysema mostly due to deficiency of the alpha 1 anti trypsin and involve the dilation of the entire acinus. Irregular emphysema is most commonly occur with irregular involvement of the acinus which is scared and inflamed. Chest x ray may reveal flattened diaphragm and hyperinflation of the chest with bullae.
Patient is treated with bronchodilators, oxyygen and advice on smoking cessation. The complication of emphysema may include pneumothorax, respiratory failure and cor pulmonale.
