Symptom finder - The causes of hypoglycemia
Symptom finder - The causes of hypoglycemia
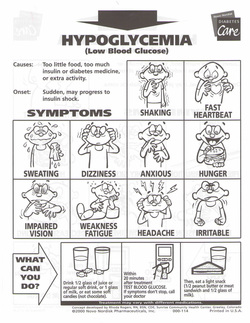
What is hypoglycemia? Hypoglycemia is when the plasma glucose level is less than 2.5 mmol/l. Hypoglycemia is an emergency condition which required urgent treatment. However, the symptoms of hypoglycemia may develop a various level of hypoglycemia. It is not specific. Hypoglycemia is detected rapidly through BM stix.
The causes of hypoglycemia are disorders of the liver such as alcohol, acute liver failure, cirrhosis and inherited glycogen storage disease. Drugs such as quinine, pentamidine, quinolones, aminoglutethimide, sulfonylurea and insulin may also cause hypoglycemia. Fibrosarcoma and pancreatic islet tumors ( insulinoma) may relate to hypoglycemia. Hypoglycemia may also associated with Addison’s disease and pituitary insufficiency. Other disorders such as Hodgkin disease ( anti - insulin receptor antibodies) and post vagotomy and drainage as well as post gastrectomy (post prandial dumping syndrome) may also cause hypoglycemia.
Hypoglycemic patient may suffer from weakness, personality changes, seizures, tremor, restlessness, drowsiness, hungers, palpitations and sweatiness.
Patient may have history of dysfunctional of pituitary / pituitary failure which is caused by infection, pituitary surgery, trauma or tumors. As an example, Addison’ disease is presented with pigmentation of the palmar crease or buccal mucosa, dizziness, weight loss and weakness. Intermittent onset of hypoglycemia is associated with islet cell tumors. Neuro cognitive and personality changes will develop.Insulinoma is defined based on the Whipple triad( attack precipitated by fasting, low blood sugar during attack and relieve of symptoms by administration of glucose). Immune mediated hypoglycemia is associated with lymphoma. Gastric surgery may lead to dumping syndrome due to high osmotic load that is delivered to the jejunum. It is important to check for evidence of liver failure.
It is vital to ask the patient regarding diabetes mellitus status and the current medication intake. The common causes of hypoglycemia is the excessive intake of oral hypoglycemic agent and insulin. Sometimes in certain cases, relatives of diabetic patient may secretly ingested the hypoglycemic agents. Athletes may also use the insulin to improve the stamina. Hypoglycemia may also occur due to excessive alcohol intake without food.
The investigations required are urea and electrolytes, blood glucose, BM stix, toxicology screen , liver function test, insulin and c peptide level, prolonged oral glucose tolerance test, pituitary hormones level, intravenous insulin suppression test, CT scan / MRI scan and arterial stimulation with venous sampling.
Retroperitoneal disease /renal failure is associated with raised urea and creatinine. Low blood glucose level is an indication of hypoglycemia. BM stix may reveal low glucose level. Toxicology screen may detect alcohol intake. Liver function test will reveal raised transaminase and bilirubin due to liver failure. Insulin level is reduced in case of pituitary failure, adrenal failure, alcohol intake or insulin receptor antibodies and non pancreatic neoplasm. Raised or normal insulin is associated with sulfonylureas treatment or insulinoma. Exogenous insulin is justified with absent of c peptide. Dumping syndrome is identified by performing prolonged oral glucose tolerance test. Pituitary hormones ( prolactin, FSH, LH, TSH and growth hormone) will reduce due to pituitary failure. Insulinoma will be detected with intravenous insulin suppression test. Insulinoma may also be detected with MRI and CT scan as well as arterial stimulation with venous sampling.
What is hypoglycemia? Hypoglycemia is when the plasma glucose level is less than 2.5 mmol/l. Hypoglycemia is an emergency condition which required urgent treatment. However, the symptoms of hypoglycemia may develop a various level of hypoglycemia. It is not specific. Hypoglycemia is detected rapidly through BM stix.
The causes of hypoglycemia are disorders of the liver such as alcohol, acute liver failure, cirrhosis and inherited glycogen storage disease. Drugs such as quinine, pentamidine, quinolones, aminoglutethimide, sulfonylurea and insulin may also cause hypoglycemia. Fibrosarcoma and pancreatic islet tumors ( insulinoma) may relate to hypoglycemia. Hypoglycemia may also associated with Addison’s disease and pituitary insufficiency. Other disorders such as Hodgkin disease ( anti - insulin receptor antibodies) and post vagotomy and drainage as well as post gastrectomy (post prandial dumping syndrome) may also cause hypoglycemia.
Hypoglycemic patient may suffer from weakness, personality changes, seizures, tremor, restlessness, drowsiness, hungers, palpitations and sweatiness.
Patient may have history of dysfunctional of pituitary / pituitary failure which is caused by infection, pituitary surgery, trauma or tumors. As an example, Addison’ disease is presented with pigmentation of the palmar crease or buccal mucosa, dizziness, weight loss and weakness. Intermittent onset of hypoglycemia is associated with islet cell tumors. Neuro cognitive and personality changes will develop.Insulinoma is defined based on the Whipple triad( attack precipitated by fasting, low blood sugar during attack and relieve of symptoms by administration of glucose). Immune mediated hypoglycemia is associated with lymphoma. Gastric surgery may lead to dumping syndrome due to high osmotic load that is delivered to the jejunum. It is important to check for evidence of liver failure.
It is vital to ask the patient regarding diabetes mellitus status and the current medication intake. The common causes of hypoglycemia is the excessive intake of oral hypoglycemic agent and insulin. Sometimes in certain cases, relatives of diabetic patient may secretly ingested the hypoglycemic agents. Athletes may also use the insulin to improve the stamina. Hypoglycemia may also occur due to excessive alcohol intake without food.
The investigations required are urea and electrolytes, blood glucose, BM stix, toxicology screen , liver function test, insulin and c peptide level, prolonged oral glucose tolerance test, pituitary hormones level, intravenous insulin suppression test, CT scan / MRI scan and arterial stimulation with venous sampling.
Retroperitoneal disease /renal failure is associated with raised urea and creatinine. Low blood glucose level is an indication of hypoglycemia. BM stix may reveal low glucose level. Toxicology screen may detect alcohol intake. Liver function test will reveal raised transaminase and bilirubin due to liver failure. Insulin level is reduced in case of pituitary failure, adrenal failure, alcohol intake or insulin receptor antibodies and non pancreatic neoplasm. Raised or normal insulin is associated with sulfonylureas treatment or insulinoma. Exogenous insulin is justified with absent of c peptide. Dumping syndrome is identified by performing prolonged oral glucose tolerance test. Pituitary hormones ( prolactin, FSH, LH, TSH and growth hormone) will reduce due to pituitary failure. Insulinoma will be detected with intravenous insulin suppression test. Insulinoma may also be detected with MRI and CT scan as well as arterial stimulation with venous sampling.
