Giardiasis symptoms

Giardiasis symptoms
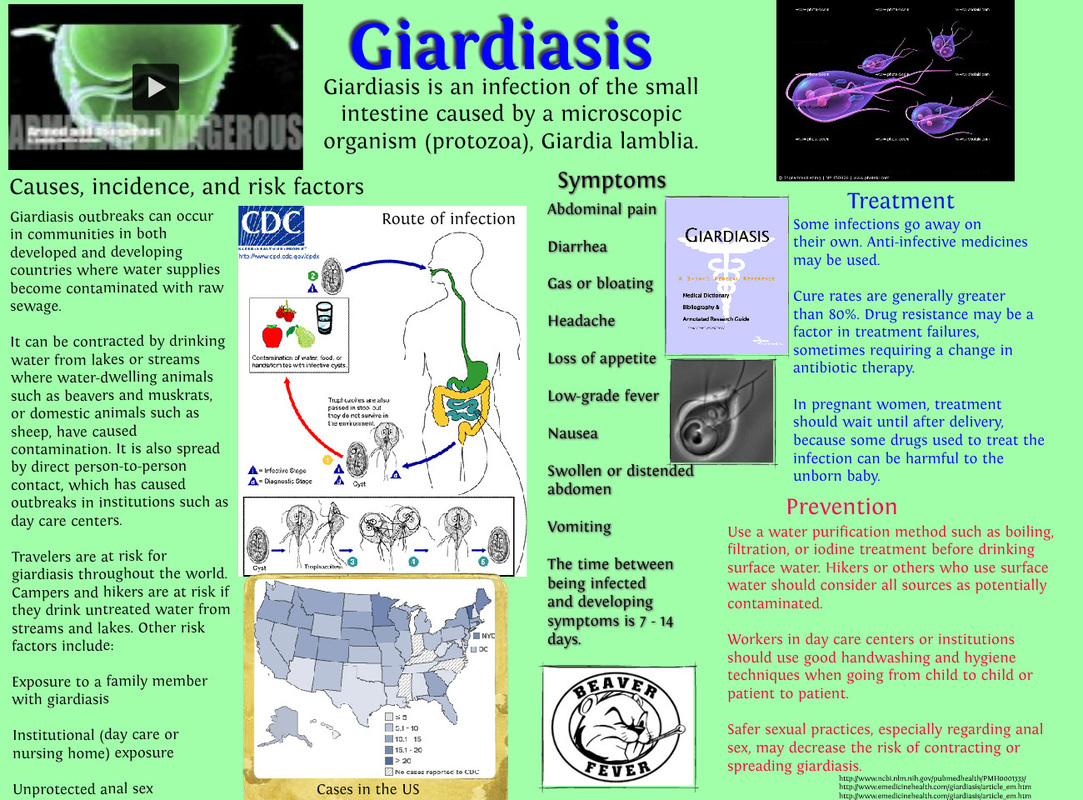
Giardiasis is an infection caused by Giardia lamblia of the upper small bowel. Giardiasis may cause diarrhea. The mode of transmission of the disease is basically involve water borne person to person or food borne.
Giardiasis is common in a place where the sanitation standards are low. Giardiasis is a globally distributed parasitosis. There are 20 000 cases of giardiasis occur from 2003 to 2006 annually in the US. Giardiasis is typically sporadic in term of infection. It may spread from person to person indirectly by ingestion of fecal contaminated food or water or from the fecal oral route. Epidemic may occur due to contamination of water supplied by gross Giardia cyst.The principal reservoir of infection are human and other animal ( wild beavers) that are infected in north of America.
The risk factors for developing giardiasis are overland travelers to far east, childcare centers, men who have sex with men and institutionalized individuals.
Generally giardiasis can be prevented by maintaining a high standard of personal hygiene and environmental sanitation. In endemic area , it is suggested to avoid any consumption of tap water by boiling the water to rapidly destroy the cyst and filtering to remove the cyst effectively. Implementation of preventive measure in residential communities of children, mentally handicapped , men who have sex with men and day care centre are suggested.
Pathologically, after ingestion of the cyst the cyst will undergo excystation which follow later by colonization of trophozoites of the upper small bowel. Disruption of the brush border may lead to diarrhea.
What is Giardia lamblia? Giardia lamblia is also known as Giardia intestinalis . Giardia lamblia exists in cyst and trophozoites forms. The cyst remain the infective form of Giardia. Cyst are infective when it passed and remain infective for few months in the water. When the cyst is ingested by a new host, the cyst will excyst in the upper gastrointestinal tract and release the trophozoites which attach to the surface of the jejunal and duodenal mucosa by theirs suckers and multiply by a binary fission. The trophozoites will later drop off from the jejunal or duodenal mucosa and mixed with the gut contents and encyst. Giardiasis is commonly assoicated with cystic fibrosis, IgA deficiency and hypochlorhydria prior to gastric surgery.
Patient usually remain asymptomatic. Children may develop high degree of tolerance to the infection. Symptoms will develop a few days ( 9 days ) to several weeks after ingestion of the cyst. Immunodeficient hosts are exposed to severe infection. The infection may progress to chronic infection. Diarrhea of subacute or acute onset may occur and diarrhea may last for weeks or months if untreated. There should be 3 - 8 bowel motions daily. The stool appears offensive, pale, bulky with mucus, flatus but not blood. Perianal soreness, urgent call to open the bowel or crampy abdominal pain may develop as well as borborygmi , bloating and steatorrhea. Patient may appear anorexic with vomiting and loss of weight. Other features such as typical abdominal distention , flatulence, gastric infection, urticaria, biliary tract disease and arthritis and anemia are rare.
Lab evaluation may include direct saline smear of stool to search for characteristic stool. Recommended to repeat the test for 3 times as 50% - 70% of cyst are found in the single stool specimen compare to 90% for repeated 3 stool specimen. Cyst appears to be 14 micrometer long, oval , 5 micrometer to 10 micrometer wide consists of 4 small nuclei and a central retractile exocysts. The number of cysts found are not related to the severity of the symptoms. Sometimes trophozoites are found in the fresh stool of the diarrhea. However, in patient with severe intense symptoms, cysts are not detected in the stool because most of the /high concentrations of trophozoites bind to the mucosa.
What is trophozoites ? It is 5 micrometer long, 3micrometer thick and 9 micrometer wide pear shaped structure with 4 pairs of flagella. ELISA ( specificity 95%- 100% and sensitivity 90% - 100% ) as well as immunofluorescent are useful in detecting Giardia antigen and commonly used. These serological methods are useful in epidemiological studies.
Entero - Test or hairy string test involved aspiration of the duodenal to recover trophozoites. This method is useful in cases where there is high index of suspicion.
Histopathology studies may reveal partial atrophy of the villus with lymphocytic infiltration of jejunum and duodenum ( intestinal biopsy ). Trophozoites can been on the surface of the bowel. The differential diagnosis of giardiasis are Crohn’s ileitis, isosporiasis, cyrptosporidiosis, Enteropathogenic E.coli infection, tropical sprue and secondary disaccharidase deficieny.
The symptomatic and asymptomatic ( children) should be treated to prevent further spread of the infection. In adult 250 - 500 mg three time daily orally for 5 days or 2- 2.5 g orally once daily for 3 days of metronidazole. At this stage, alcohol intake should be stopped as metronidazole and alcohol interaction may lead to flushing and headache. The dose is modified into 5mg per kg three times daily for seven days. 500 mg nitazoxanide twice daily for 5 days has similar effect as metronidazole. 2 g tinidazole is also useful as an alternative.
The second stage of treatment include 400 mg albendazole orally daily for 5 days.100 mg Mepacrine ( quinacrine) orally 5- 7 days on adult and 2 mg per kg twice a day for children up to 5 - 7 days. Furazolidone carries an efficacy up to 80%. It should be used with cautious as it may lead to hemolysis in patient with G 6 PD deficiency. 10% - 20% of failure rate of treatment is expected. The infection is eradicated by repeating treatment for a longer course or change to another appropriate drug. Combination of 2 drugs shoul also be considered ( such as mepacrine and metronidazole) if other drug regimens fail. Repeated relapse may occur due to infection from close contact with asymptomatic infected person or other family member. After treatment, diarrhea is still persists due to concomitant tropical sprue or secondary lactose intolerance.
Pregnant woman with severe case of giardiasis should be considered 2.5- 3.5 mg per kg paromomycin orally for 7 days in 3 divided doses. Metronidazole is avoided in pregnant woman due to its teratogenic effect.
The complication of giardiasis are hypogammaglobulinemia, weight loss, malabsorption and steatorrhea.
The patient’s body weight and symptoms are monitored. Stool examination is performed. Asymptomatic infection is associated with patient high degree of tolerance. Symptomatic condition may last for weeks or months and the patient will be self limiting. Patient may also has a concomitant bacterial infection of his bowel.
Giardiasis is an infection caused by Giardia lamblia of the upper small bowel. Giardiasis may cause diarrhea. The mode of transmission of the disease is basically involve water borne person to person or food borne.
Giardiasis is common in a place where the sanitation standards are low. Giardiasis is a globally distributed parasitosis. There are 20 000 cases of giardiasis occur from 2003 to 2006 annually in the US. Giardiasis is typically sporadic in term of infection. It may spread from person to person indirectly by ingestion of fecal contaminated food or water or from the fecal oral route. Epidemic may occur due to contamination of water supplied by gross Giardia cyst.The principal reservoir of infection are human and other animal ( wild beavers) that are infected in north of America.
The risk factors for developing giardiasis are overland travelers to far east, childcare centers, men who have sex with men and institutionalized individuals.
Generally giardiasis can be prevented by maintaining a high standard of personal hygiene and environmental sanitation. In endemic area , it is suggested to avoid any consumption of tap water by boiling the water to rapidly destroy the cyst and filtering to remove the cyst effectively. Implementation of preventive measure in residential communities of children, mentally handicapped , men who have sex with men and day care centre are suggested.
Pathologically, after ingestion of the cyst the cyst will undergo excystation which follow later by colonization of trophozoites of the upper small bowel. Disruption of the brush border may lead to diarrhea.
What is Giardia lamblia? Giardia lamblia is also known as Giardia intestinalis . Giardia lamblia exists in cyst and trophozoites forms. The cyst remain the infective form of Giardia. Cyst are infective when it passed and remain infective for few months in the water. When the cyst is ingested by a new host, the cyst will excyst in the upper gastrointestinal tract and release the trophozoites which attach to the surface of the jejunal and duodenal mucosa by theirs suckers and multiply by a binary fission. The trophozoites will later drop off from the jejunal or duodenal mucosa and mixed with the gut contents and encyst. Giardiasis is commonly assoicated with cystic fibrosis, IgA deficiency and hypochlorhydria prior to gastric surgery.
Patient usually remain asymptomatic. Children may develop high degree of tolerance to the infection. Symptoms will develop a few days ( 9 days ) to several weeks after ingestion of the cyst. Immunodeficient hosts are exposed to severe infection. The infection may progress to chronic infection. Diarrhea of subacute or acute onset may occur and diarrhea may last for weeks or months if untreated. There should be 3 - 8 bowel motions daily. The stool appears offensive, pale, bulky with mucus, flatus but not blood. Perianal soreness, urgent call to open the bowel or crampy abdominal pain may develop as well as borborygmi , bloating and steatorrhea. Patient may appear anorexic with vomiting and loss of weight. Other features such as typical abdominal distention , flatulence, gastric infection, urticaria, biliary tract disease and arthritis and anemia are rare.
Lab evaluation may include direct saline smear of stool to search for characteristic stool. Recommended to repeat the test for 3 times as 50% - 70% of cyst are found in the single stool specimen compare to 90% for repeated 3 stool specimen. Cyst appears to be 14 micrometer long, oval , 5 micrometer to 10 micrometer wide consists of 4 small nuclei and a central retractile exocysts. The number of cysts found are not related to the severity of the symptoms. Sometimes trophozoites are found in the fresh stool of the diarrhea. However, in patient with severe intense symptoms, cysts are not detected in the stool because most of the /high concentrations of trophozoites bind to the mucosa.
What is trophozoites ? It is 5 micrometer long, 3micrometer thick and 9 micrometer wide pear shaped structure with 4 pairs of flagella. ELISA ( specificity 95%- 100% and sensitivity 90% - 100% ) as well as immunofluorescent are useful in detecting Giardia antigen and commonly used. These serological methods are useful in epidemiological studies.
Entero - Test or hairy string test involved aspiration of the duodenal to recover trophozoites. This method is useful in cases where there is high index of suspicion.
Histopathology studies may reveal partial atrophy of the villus with lymphocytic infiltration of jejunum and duodenum ( intestinal biopsy ). Trophozoites can been on the surface of the bowel. The differential diagnosis of giardiasis are Crohn’s ileitis, isosporiasis, cyrptosporidiosis, Enteropathogenic E.coli infection, tropical sprue and secondary disaccharidase deficieny.
The symptomatic and asymptomatic ( children) should be treated to prevent further spread of the infection. In adult 250 - 500 mg three time daily orally for 5 days or 2- 2.5 g orally once daily for 3 days of metronidazole. At this stage, alcohol intake should be stopped as metronidazole and alcohol interaction may lead to flushing and headache. The dose is modified into 5mg per kg three times daily for seven days. 500 mg nitazoxanide twice daily for 5 days has similar effect as metronidazole. 2 g tinidazole is also useful as an alternative.
The second stage of treatment include 400 mg albendazole orally daily for 5 days.100 mg Mepacrine ( quinacrine) orally 5- 7 days on adult and 2 mg per kg twice a day for children up to 5 - 7 days. Furazolidone carries an efficacy up to 80%. It should be used with cautious as it may lead to hemolysis in patient with G 6 PD deficiency. 10% - 20% of failure rate of treatment is expected. The infection is eradicated by repeating treatment for a longer course or change to another appropriate drug. Combination of 2 drugs shoul also be considered ( such as mepacrine and metronidazole) if other drug regimens fail. Repeated relapse may occur due to infection from close contact with asymptomatic infected person or other family member. After treatment, diarrhea is still persists due to concomitant tropical sprue or secondary lactose intolerance.
Pregnant woman with severe case of giardiasis should be considered 2.5- 3.5 mg per kg paromomycin orally for 7 days in 3 divided doses. Metronidazole is avoided in pregnant woman due to its teratogenic effect.
The complication of giardiasis are hypogammaglobulinemia, weight loss, malabsorption and steatorrhea.
The patient’s body weight and symptoms are monitored. Stool examination is performed. Asymptomatic infection is associated with patient high degree of tolerance. Symptomatic condition may last for weeks or months and the patient will be self limiting. Patient may also has a concomitant bacterial infection of his bowel.