Medicine Notes - Clinical Procedures - Peak Expiratory Flow Measurements

Peak expiratory flow measurements
Peak expiratory flow measurement is considered in identifying and assessing the severity of asthma ( acute asthmatic attack) or chronic obstructive pulmonary disease.
Peak expiratory flow measurement is also useful in identifying any reversibility of asthma or chronic obstructive pulmonary disease due to inhaled bronchodilator. The reversibility is considered if there is an improvement of more than 60L/min after treatment with inhaled bronchodilator.
Peak expiratory flow measurement is also important for patient who need to record the peak expiratory flow rate in certain time period ( assessing the diurnal variation).
A peak flow meter and clean disposable mouth piece is considered in measuring the peak expiratory flow rate or PEFR.
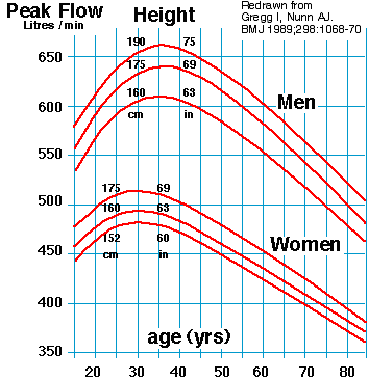
The highest value of peak expiratory flow rate is considered to be recorded in L/min. The highest value of peak expiratory flow rate can also be considered as a percentage of the best predicted or previous PEFR. The normal value of peak expiratory flow rate varies according to the patient’s gender, age and height. To avoid confusion, the value need to be compared with the patient previous best PEFR value.
First, make sure the patient is sitting upright or standing.
Prepare the peak flow meter. Make sure that the peak flow meter is hold correctly and not covering the meter reader/marker. The meter also need to be set at 0.
The patient, then need to take a deep breath in. Hold the mouthpiece in the mouth and seal the lip tightly around the mouthpiece.
The patient next, need to blow out as fast and hard as possible. It is more like blowing out a candle. Patient who develop difficulty may require brief demonstration on how it should be performed.
The procedure is repeated and the the best of the 3 efforts are recorded. Further measurement may be required if the patient unable to achieve a value within 40L/min after two attempts.
The common contraindication of measuring peak flow expiratory rate is in severe respiratory distress condition such as life threatening asthma. In this case, the main priority is to stabilize the patient first. (airway, breathing, circulation).
Peak expiratory flow measurement is considered in identifying and assessing the severity of asthma ( acute asthmatic attack) or chronic obstructive pulmonary disease.
Peak expiratory flow measurement is also useful in identifying any reversibility of asthma or chronic obstructive pulmonary disease due to inhaled bronchodilator. The reversibility is considered if there is an improvement of more than 60L/min after treatment with inhaled bronchodilator.
Peak expiratory flow measurement is also important for patient who need to record the peak expiratory flow rate in certain time period ( assessing the diurnal variation).
A peak flow meter and clean disposable mouth piece is considered in measuring the peak expiratory flow rate or PEFR.
The highest value of peak expiratory flow rate is considered to be recorded in L/min. The highest value of peak expiratory flow rate can also be considered as a percentage of the best predicted or previous PEFR. The normal value of peak expiratory flow rate varies according to the patient’s gender, age and height. To avoid confusion, the value need to be compared with the patient previous best PEFR value.
First, make sure the patient is sitting upright or standing.
Prepare the peak flow meter. Make sure that the peak flow meter is hold correctly and not covering the meter reader/marker. The meter also need to be set at 0.
The patient, then need to take a deep breath in. Hold the mouthpiece in the mouth and seal the lip tightly around the mouthpiece.
The patient next, need to blow out as fast and hard as possible. It is more like blowing out a candle. Patient who develop difficulty may require brief demonstration on how it should be performed.
The procedure is repeated and the the best of the 3 efforts are recorded. Further measurement may be required if the patient unable to achieve a value within 40L/min after two attempts.
The common contraindication of measuring peak flow expiratory rate is in severe respiratory distress condition such as life threatening asthma. In this case, the main priority is to stabilize the patient first. (airway, breathing, circulation).