Abscess Symptoms - Perirectal Abscess
Perirectal Abscess
Perirectal abscess is also known as anorectal abscess, rectal abscess and perianal abscess.
The underlying condition associated with perirectal abscess are malignancy or leukemia,immune deficiency,diabetes mellitus,recent surgery and steroid therapy.
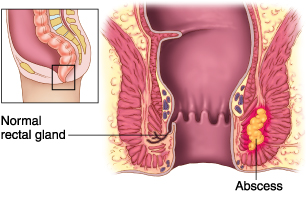
A perirectal abscess is a localized inflammatory process that can be associated with infections of soft tissue and anal glands based on anatomic location. Perianal and perirectal abscesses may be simple or complex, causing suppuration. Infections in these spaces may be classified as superficial perianal or perirectal with involvement in the following anatomic spaces: ischiorectal, intersphincteric, perianal, and supralevator. The Parks classification of anorectal abscess is subdivided in intersphincteric, transsphincteric, suprasphincteric, and extrasphincteric abscess.
The common symptoms and signs of perirectal abscess are localized perirectal or anal pain—often worsened with movement or straining,perirectal erythema or cellulitis, perirectal mass by inspection or palpation,fever and signs of sepsis with deep abscess
as well as urinary retention.
The common causes of perirectal abscess are polymicrobial aerobic and anaerobic bacteria involving one of the anatomic spaces , often associated with localized
trauma. Predominant anaerobic bacteria:. Bacteroides fragilis, Peptostreptococcus spp., Prevotella spp, Porphyromonas spp.,Clostridium spp. and Fusobacterium spp.
Predominant aerobic bacteria are Streptococcus spp., Escherichia coli and Enterococcus spp.
The differential diagnosis of perirectal abscess are neutropenic enterocolitis, Crohn’s disease (inflammatory bowel disease), Pilonidal disease, Hidradenitis suppurativa tuberculosis or actinomycosis; Chagas’ disease,cancerous lesions, chronic anal fistula
rectovaginal fistula,proctitis—often STD-associated, including: syphilis, gonococcal, chlamydia, chancroid, condylomata acuminata and AIDS-associated: Kaposi’s sarcoma, lymphoma and cytomegalovirus.
The investigation techniques for perirectal abscess are examination of rectal, perirectal/perineal areas to rule out necrotic process and crepitance suggesting deep tissue involvement.
Other form of investigations are local aerobic and anaerobic culture Blood cultures if toxic, febrile, or compromised. Possible sigmoidoscopy
Usually imaging studies not indicated unless extensive disease abscess but can include CT scan.
The treatment of perirectal abscess may include incision and drainage of abscess debridement if necrotic tissue, rule out need for fistulectomy, local wound care—packing
Sitz baths and antibiotic treatment which is directed toward coverage for mixed skins and enteric flora.
Perirectal abscess is also known as anorectal abscess, rectal abscess and perianal abscess.
The underlying condition associated with perirectal abscess are malignancy or leukemia,immune deficiency,diabetes mellitus,recent surgery and steroid therapy.
A perirectal abscess is a localized inflammatory process that can be associated with infections of soft tissue and anal glands based on anatomic location. Perianal and perirectal abscesses may be simple or complex, causing suppuration. Infections in these spaces may be classified as superficial perianal or perirectal with involvement in the following anatomic spaces: ischiorectal, intersphincteric, perianal, and supralevator. The Parks classification of anorectal abscess is subdivided in intersphincteric, transsphincteric, suprasphincteric, and extrasphincteric abscess.
The common symptoms and signs of perirectal abscess are localized perirectal or anal pain—often worsened with movement or straining,perirectal erythema or cellulitis, perirectal mass by inspection or palpation,fever and signs of sepsis with deep abscess
as well as urinary retention.
The common causes of perirectal abscess are polymicrobial aerobic and anaerobic bacteria involving one of the anatomic spaces , often associated with localized
trauma. Predominant anaerobic bacteria:. Bacteroides fragilis, Peptostreptococcus spp., Prevotella spp, Porphyromonas spp.,Clostridium spp. and Fusobacterium spp.
Predominant aerobic bacteria are Streptococcus spp., Escherichia coli and Enterococcus spp.
The differential diagnosis of perirectal abscess are neutropenic enterocolitis, Crohn’s disease (inflammatory bowel disease), Pilonidal disease, Hidradenitis suppurativa tuberculosis or actinomycosis; Chagas’ disease,cancerous lesions, chronic anal fistula
rectovaginal fistula,proctitis—often STD-associated, including: syphilis, gonococcal, chlamydia, chancroid, condylomata acuminata and AIDS-associated: Kaposi’s sarcoma, lymphoma and cytomegalovirus.
The investigation techniques for perirectal abscess are examination of rectal, perirectal/perineal areas to rule out necrotic process and crepitance suggesting deep tissue involvement.
Other form of investigations are local aerobic and anaerobic culture Blood cultures if toxic, febrile, or compromised. Possible sigmoidoscopy
Usually imaging studies not indicated unless extensive disease abscess but can include CT scan.
The treatment of perirectal abscess may include incision and drainage of abscess debridement if necrotic tissue, rule out need for fistulectomy, local wound care—packing
Sitz baths and antibiotic treatment which is directed toward coverage for mixed skins and enteric flora.